Table of Contents
- The Origins of HRT
- Reframing the Transition
- Robert Wilson, Premarin, and the Sales Campaign
- The Disruptors
- Hormone-Disrupting Exposures
- 1) Plastics & Food Contact Chemicals
- 2) PFAS & Grease/Water-Resistant Chemicals
- 3) Fragrance & Personal Care Chemicals
- 4) Cleaning Agents, Surfactants & Preservatives
- 5) Agricultural Chemicals
- 6) Persistent Pollutants & Heavy Metals
- 7) Solvents & Penetration Enhancers
- 8) Stimulants & Metabolic Modifiers
- 9) Synthetic Vitamins & Fortification Additives
- 10) Pharmaceutical & Hormone-Active Drugs
- 11) Textiles, Synthetic Clothing & Skin-Contact Plastics
- 12) Menstrual, Feminine & Sexual Health Products
- 13) Spermicides & Sexual Lubricants (the actual cause of a STI)
- 14) Paper Products & Bleaching/Processing Residues
- 15) Home Furnishings, Foam & Fire Retardant Fabrics
- 16) Air, Smoke & Combustion Byproducts
- 17) Food Service Packaging & Heat-Driven Migration (Exposure Amplifier)
- 18) Water Contaminants & Treatment Byproducts
- 19) “Wellness” Product Contaminants & Adulteration
- 20) Oncology & Radiation Exposure
- 21) Salon, Nail & Hair Product Chemicals
- 22) Candles, Air Scenting & Indoor Fragrance Emissions
- Wake Up, You have been Played (Again)
- So no, Virginia, there is no such thing as Santa Claus, and no, there is no such thing as menopause. You are TOXIC, and your toxic load has hit critical mass because you lost your primary detox pathway when you stopped menstruating. Now all the garbage you infuse yourself with is stuck in your body, looping around, accumulating in your burgeoning fat storage. You have become a garbage dump, a chemtrail, and a forever chemical wrapped up in yoga pants.
- The Feedback Loop Consequence
- Conclusion
- Side Note
The Origins of HRT

In the first article, I questioned why menopause is seen as a set of symptoms and as something to medicate. I also looked at how menopause and perimenopause have been framed as a medical crisis, rather than a biological transition. Symptoms commonly linked to “hormonal chaos” may not always start with ovarian failure. We explored how modern culture reinforces this narrative and how it benefits the economy by rebranding normal aging as a deficiency. The invented deficiency delusion is the latest wave of medical interference and drug management.
By the way, I found 141 movies about menopause, in which the main character goes through menopause as a main theme. The list below is only 41; imagine 2 more galleries filled with movies. The worst are the comedians, which is why nearly all older female comics make menopause a main theme in their shows. This is how they infuse a delusional construct into society, making it real. They are the alchemists of the mind.
In the second article, I examined how hormone therapy fits into a larger growth model: expand the diagnosis, lower the age of entry, normalize intervention, and remain ever-present across decades. We reviewed how steroid hormones are made, how feedback loops regulate them, and how lab values capture only a fleeting snapshot of a continuous rhythmic system. We explored what happens when external hormones override internal signaling, and why fluctuating lab results do not mean a broken body.
Now we need to step back even further.
Before hormone therapy became a subscription model, before movies and celebrity testimonials reframed risk as empowerment, before “perimenopause” became a marketing keyword, there was a moment in history when menopause itself was redefined. It did not emerge from ancient medicine. It was not discovered in a laboratory. It was constructed, slowly at first, then aggressively, through books, Hollywood, media campaigns, comedians, and pharmaceutical alliances that reframed aging ovaries as endocrine failure.
To understand where we are now, we have to understand how that reframing began.
Reframing the Transition
In the nineteenth century, a savvy snake-oil salesman, aka French physician Charles Pierre Louis de Gardanne, is credited with formalizing the term menopause. In 1821, he published an article describing what he called “la ménopause,” combining the Greek words for month and cessation. Once named, it could be discussed as a defined stage rather than an undefined passage, and then pathologized to increase his revenue in private practice.
De Gardanne described a constellation of symptoms that he associated with the end of menstruation, including nervousness, heat sensations, and mood changes. He wrote within the medical framework of his time, which often linked women’s health to the uterus and ovaries in broad and sometimes speculative ways. His descriptions were observational, but grouping symptoms under a single heading was significant.
As nineteenth-century medicine evolved, physicians increasingly sought to compartmentalize the female customer by organizing bodily changes into identifiable syndromes. The newly emerging discipline of gynecology focused heavily on reproductive anatomy and function. Within that context, the cessation of menses was not just an absence of bleeding but a physiological event that could be analyzed, monitored, and, of course, monetized.
French and later European physicians contributed to literature that treated menopause as a clinical stage. This included potential complications. Many women moved through midlife without intervention. Yet medical texts increasingly framed the transition as something that could destabilize the nervous system or predispose women to ailments. The language varied, but the pattern was consistent. A life phase became a medical chapter. Once women hear it from the authority they trust, they become it.
This intellectual shift did not immediately produce pharmaceutical solutions. Synthetic hormones did not yet exist. However, the groundwork was laid, as with all the other gold rushes of newly discovered “syndromes”. If a set of symptoms could be grouped and named, it could later be measured. If it could be measured, it could eventually be targeted. These guys were simply laying the foundation and framework for a burgeoning industry.
By the time endocrinology matured in the twentieth century, a conceptual container was already in place. The naming of menopause created a lens through which natural variation could now be interpreted as imbalance. That interpretive shift would become far more consequential once hormone therapy entered the picture.
Robert Wilson, Premarin, and the Sales Campaign
In 1966, Dr. Robert A. Wilson published Feminine Forever. This book reframed estrogen therapy as the solution to what he called an estrogen deficiency disease. Wilson argued that menopause meant systemic deterioration caused by hormone loss. He claimed this decline could be prevented with lifelong estrogen use.
He described untreated women in terms that equated ovarian aging with demise, decay, and feminine devastation. He wrote that postmenopausal women were, in his words, “castrates.” He claimed that without estrogen therapy, women would become physically diminished, emotionally unstable, and socially irrelevant. He positioned estrogen not as symptom relief for severe cases, but as preservation of femininity itself.
The framing aligned precisely with an existing product.
Premarin, a conjugated equine estrogen derived from the urine of pregnant mares, had already been developed and marketed by Wyeth. The name itself was a contraction of pregnant mare urine. By the 1960s, it was one of the few available estrogen formulations suitable for long-term prescribing. What it lacked was a broad, fear-driven narrative directed at healthy midlife women.
Wilson was hired by Big Pharma and supplied that narrative. His educational foundation and promotional work were financially supported by Wyeth. The relationship was not prominently disclosed in early public discussions. The book served as persuasive mass communication at a time when direct-to-consumer pharmaceutical advertising had not yet dominated television.
The argument was simple. First, define estrogen reduction and ovarian aging as pathology. Next, present estrogen as the solution for complete feminine restoration. Then expand the eligible population from women with severe symptoms to all women entering midlife. Wilson recommended using estrogen from menopause until death to maintain tissue tone, mood stability, sexual responsiveness, and overall vitality. When I started in locked psych wards and residential treatment, every woman was taking Premarin and Provera. First, make them crazy with the horse urine. Then, lock them up and give them chemical restraints for the rest of their lives. A perfect business model.
Within a few years, evidence linked unopposed estrogen therapy to a significant increase in endometrial cancer rates. Prescribing practices adjusted to include progestins to counteract uterine stimulation. The commercial relationship between the author and the manufacturer later became widely known, reinforcing the view that Feminine Foreveroperated as a marketing vehicle.
Premarin prescriptions rose sharply after publication. Estrogen soon became one of the most prescribed medications in the United States. The cultural understanding of menopause shifted in parallel. Hormone therapy moved from selective intervention to routine and unquestioned therapy.

Hormone signaling today unfolds in a landscape saturated by chemical exposures, dietary shifts, and lifestyle pressures not present at the same scale when Feminine Forever was published. Remember, HRT is an industry that needs steady profits. It expands menopause to include perimenopause, then hormonal disorders, then gender and alphabet army disorders. The hungry ghost is never satisfied until every living woman takes hormones. For those reluctant to sip the tea, there are options you may not know. The Pugh photo shows obvious symbols: spilling the tea, the black-and-white checkered floor—a favorite of the Baphomet cult. The tea represents taking hormones for MTF or FTM. Whether true or not, we may never know. Men drinking pregnant horse urine is one way to develop female traits, similar to drinking urine from girls on birth control pills.
The Disruptors
Before blaming ovarian decline for ANY midlife symptoms, we should ask what else influences hormone signaling. The endocrine system functions through feedback loops. The brain signals the ovaries. The ovaries produce hormones that signal the brain. Production adjusts in response to circulating levels.
When external compounds enter the system and bind to hormone receptors or alter metabolism, the feedback loop responds. If estrogenic activity increases from outside sources, the brain may reduce its own stimulation. If stress hormones remain chronically elevated, reproductive signaling can be suppressed. When liver detoxification pathways are burdened, hormone clearance shifts. The system adapts to inputs, whether they originate in ovaries or the environment.
Modern women are not operating in a biologically neutral environment.
Hormone-Disrupting Exposures
No, it’s not the “menopause,” ma’am, it’s YOU.
1) Plastics & Food Contact Chemicals
Bisphenols (BPA, BPS, BPF), Phthalates (DEHP, DBP, DEP, DiNP/DiDP), Styrene, Plasticizers, Microplastics/Nanoplastics
What / how formed:
Petrochemical-derived monomers and plasticizers are used to make hard and flexible plastics; microplastics form from wear, heat, washing, and breakdown.
Endocrine relevance:
Bisphenols mimic estrogen and disrupt androgen signaling. Phthalates are anti-androgenic and associated with reduced testosterone and altered reproductive development. Microplastics can carry other endocrine-active pollutants, thereby increasing internal exposure.
Common exposure:
Canned food linings • All forms of Plastic-THERE IS NO BPA FREE OR SAFE PLASTIC, IT IS A MARKETING SCAM. • Plastic containers/wrap • Bottled water • Microwaving in plastic • Hot drinks in lined cups • Baby bottles/sippy cups • Receipts/recycled paper • Food storage lids
2) PFAS & Grease/Water-Resistant Chemicals
PFOS, PFOA, PFHxS, PFNA, GenX, Fluorotelomers, Fluorinated polymers
What / how formed:
Fluorinated industrial compounds engineered to resist grease, stains, and heat; carbon–fluorine bonds make them persist and bioaccumulate.
Endocrine relevance:
Associated with thyroid disruption, altered reproductive hormones, reduced fertility markers, and metabolic hormone changes.
Common exposure:
Nonstick cookware • Grease-resistant takeout wrappers • Fast-food packaging • Microwave popcorn bags • Waterproof/stain-resistant clothing • Carpets/upholstery treatments • Contaminated water
3) Fragrance & Personal Care Chemicals
“Fragrance/Parfum” blends, Phthalates (DEP), Parabens, Synthetic musks (HHCB/AHTN), UV filters (oxybenzone/octinoxate), Siloxanes (D4/D5/D6)
What / how formed:
Proprietary petrochemical scent blends, preservatives, stabilizers, and musks are synthesized for longevity and texture.
Endocrine relevance:
Can act as weak estrogen mimics/anti-androgens, disrupt thyroid signaling, and contribute to chronic low-dose hormone load through skin absorption and inhalation.
Common exposure:
Perfume/cologne • ALL Deodorant even the “healthy ones”• Commercial Lotions • Shampoo/conditioner • Makeup/lipstick • Hair products • SPF cosmetics • Body sprays
4) Cleaning Agents, Surfactants & Preservatives
Quats (benzalkonium chloride/DDAC), Ethoxylated surfactants (PEGs, SLES/“laureth”), 1,4-dioxane (byproduct), Formaldehyde + releasers (DMDM hydantoin, etc.), Triclosan/triclocarban
What / how formed:
Synthesized to kill microbes, emulsify oils, and preserve shelf life; some processes (ethoxylation) can create byproducts.
Endocrine relevance:
Can irritate mucosal barriers and skin (increasing absorption), alter microbiome signaling, and add to endocrine burden through chronic exposure—especially via daily household use.
Common exposure:
Laundry detergent • Hand Sanitizer • Fabric softener • Dryer sheets • Dish soap • Hand soap • Disinfectant wipes/sprays • Bathroom cleaners • Wet wipes • “Antibacterial” products
5) Agricultural Chemicals
Herbicides (atrazine, 2,4-D, glyphosate formulations), Insecticides (organophosphates, pyrethroids, neonicotinoids)
What / how formed:
Industrial agrochemicals are synthesized to disrupt plant or insect biological pathways; residues persist in soil, dust, and water.
Endocrine relevance:
It can disrupt reproductive hormone signaling, thyroid function, and developmental endocrine programming; chronic low-dose exposure can shift fertility and puberty timing.
Common exposure:
Conventional produce • Grains/legumes • Lawn treatments • Drift exposure • Household dust near agriculture • Contaminated water • All Hired Landscaping Services
6) Persistent Pollutants & Heavy Metals
Dioxins, PCBs, PAHs, Mercury, Lead, Cadmium, Arsenic
What / how formed:
Industrial combustion byproducts and legacy industrial chemicals; heavy metals mobilized through mining/industry, and accumulating in tissues.
Endocrine relevance:
Disrupt thyroid hormone transport/production, impair ovarian/testicular function, reduce testosterone, alter estrogen metabolism, and affect cortisol and glucose regulation.
Common exposure:
Large predatory fish (tuna-type, swordfish-type) • Rice/rice products (arsenic) • Cocoa/chocolate (cadmium) • Old paint/soil • Industrial air • Contaminated water
7) Solvents & Penetration Enhancers
Alcohol (ethanol), DMSO, Turpentine (terpenes), Glycol ethers, Chlorine dioxide
What / how formed:
Alcohol from fermentation/distillation. DMSO from wood pulp processing. Turpentine is distilled from pine resin. Glycol ethers and chlorine dioxide are industrial solvents/oxidizers.
Endocrine relevance:
Alcohol increases aromatase (testosterone → estrogen), suppresses testosterone, and impairs fertility with repeated exposure. DMSO and some solvents alter estrogen receptor activity and reproductive cell development and increase absorption of other chemicals through the skin. Liver stress changes hormone clearance, shifting testosterone/estrogen balance.
Common exposure:
Alcoholic beverages • Mouthwash • Tinctures • Essential oil concentrates • Alternative “detox” protocols • Paint/solvent fumes • Cleaning chemicals • Essential Oils (most are synthetic chemicals in carrier oils like doTerrible)
8) Stimulants & Metabolic Modifiers
Caffeine (and related methylxanthines)
What / how formed:
Plant alkaloids extracted from coffee/tea/cacao or synthesized for supplements and drinks.
Endocrine relevance:
Shift’s cortisol rhythm and adrenal signaling influence insulin sensitivity and affect reproductive hormone balance indirectly through stress pathways.
Common exposure:
Coffee • Energy drinks • Pre-workouts • Tea • Chocolate
9) Synthetic Vitamins & Fortification Additives
All vitamins are synthetic chemicals made in the same way as prescription drugs. Some are more destructive to hormones, but they all are. Vitamin D3 (cholecalciferol), Vitamin D2 (ergocalciferol), Vitamin A (retinyl palmitate/acetate), Vitamin E (dl-alpha-tocopherol acetate), Vitamin C (ascorbic acid), Vitamin B6 (pyridoxine HCl), Vitamin B12 (cyanocobalamin), Vitamin B9 (folic acid), B1 (thiamine), B2 (riboflavin), B3 (niacinamide), Iodine salts (potassium iodide/iodate), Biotin (vitamin B7)
What / how formed:
Industrial isolates are produced via chemical reactions with chemicals such as coal tar, hydrochloric acid, nail polish remover, and/or petrochemical synthesis, and are stabilized for shelf life; added to most packaged foods or sold as supplements.
Endocrine relevance:
Isolated compounds can alter receptor signaling and hormone feedback loops (thyroid, cortisol, sex hormones) depending on dose and context. Retinoids intersect with thyroid signaling. Biotin can distort hormone lab tests (TSH, cortisol, testosterone, estradiol), creating false “diagnoses.” Vitamin D and E act in very similar ways to Estrogen.
Vitamin D
“Vitamin D” functions as a hormone, and the active form binds to the “vitamin D” receptor and influences gene expression in reproductive tissues. It interacts with enzymes involved in steroid metabolism, including aromatase, thereby shifting circulating estradiol and progesterone levels rather than merely “supporting” them.
Vitamin E
Vitamin E interacts with estrogen receptors and influences estrogen signaling. Because different tocopherols and tocotrienols act differently, high-dose supplementation can influence estrogen-responsive tissues depending on the dose and context.
Common exposure:
Multivitamins • Prenatals • Fortified flour/cereal • Fortified plant milks • “Hair/skin/nails” products • Energy drinks • “Immune” powders/gummies
10) Pharmaceutical & Hormone-Active Drugs
Hormonal contraceptives, Anabolic steroids, Corticosteroids, SSRIs/SNRIs, Antipsychotics, Beta-blockers, Diuretics, Anticonvulsants, Antibiotics (rifampin), Antifungals (ketoconazole), NSAIDs, H2 blockers (cimetidine/Tagamet), Ivermectin, Hydroxychloroquine, Finasteride/anti-androgens
What / how formed:
Synthetic receptor-targeting compounds developed through medicinal chemistry. Designed to bind or modulate endocrine or neuroendocrine pathways.
Endocrine relevance:
Can suppress testosterone, alter estrogen/progesterone signaling, change cortisol output, affect thyroid conversion, shift glucose/insulin hormones, or speed/slow hormone metabolism in the liver—impacting fertility, libido, mood, and menstrual cycling depending on duration and dose.
Common exposure:
Birth control (oral, injectable, IUD) • Steroid meds • Antidepressants • Blood pressure meds • Anti-seizure meds • Antibiotics/antifungals • Antiparasitics • Autoimmune therapies
11) Textiles, Synthetic Clothing & Skin-Contact Plastics
Polyester, Nylon, Spandex/Elastane, Polyurethane, PFAS textile finishes, Flame retardants (organophosphates), Textile dyes (azo dyes, heavy metal pigments)
What / how formed:
Petroleum-based polymers are spun into fibers and treated with finishes (water- and wrinkle-resistant) and antimicrobial coatings during manufacturing.
Endocrine relevance:
Continuous skin contact increases exposure to additives (phthalates, PFAS finishes, flame retardants). Heat and sweating increase transfer, and endocrine-active additives can contribute to hormone burden (thyroid, testosterone/estrogen balance).
Common exposure:
Athletic wear • Yoga pants • Compression wear • Underwear/bras • Socks • Bedding • Swimwear • Rain jackets • “Stain resistant” uniforms • Car upholstery
12) Menstrual, Feminine & Sexual Health Products
Fragrance chemicals, phthalates, parabens, PFAS (in some product types/lines), formaldehyde-releaser residues, adhesives/additive polymers
What / how formed:
Absorbent fibers, adhesives, coatings, and fragrances are industrially processed and stabilized; some products use water- and grease-resistant finishes.
Endocrine relevance:
Vaginal and vulvar tissue has high absorption. Chronic low-dose exposure to endocrine-active additives can affect fertility signaling, inflammation, and hormone balance.
Common exposure:
Tampons • Pads/liners • Period underwear • Feminine washes • Scented products • Condom lubricants •Toilet Paper
13) Spermicides & Sexual Lubricants (the actual cause of a STI)
Nonoxynol-9, preservatives, fragrance compounds, polyethylene glycols (PEGs)
What / how formed:
Surfactant-based spermicides and gel formulations are designed to disrupt membranes and are stabilized with preservatives and thickeners.
Endocrine relevance:
Can irritate mucosa, alter local microbiome, and increase permeability—raising exposure to endocrine-active compounds and inflammatory hormone shifts.
Common exposure:
Spermicidal gels/films • Some lubricants • Barrier contraceptive products
14) Paper Products & Bleaching/Processing Residues
BPA/BPS from recycled pulp contamination, fragrance additives, and bleaching byproducts
What / how formed:
Recycled paper streams can carry thermal-receipt bisphenols; bleaching and fragrance treatments add additional chemical load.
Endocrine relevance:
Bisphenols are estrogen-active; repeated skin contact adds to cumulative exposure.
Common exposure:
Toilet paper • Paper towels • Napkins • Facial tissues • Receipts
15) Home Furnishings, Foam & Fire Retardant Fabrics
Flame retardants (PBDEs/organophosphates), PFAS finishes, VOCs (toluene/xylene), plasticizers
What / how formed:
Foams and textiles are treated to meet fire codes and stain resistance; additives migrate out and concentrate in dust.
Endocrine relevance:
Dust exposure is a major chronic route of exposure to hormone-active chemicals (thyroid disruption, anti-androgen effects, altered puberty/fertility signals).
Common exposure:
Mattresses • Couch foam • Carpets • Curtains • Car interiors • Electronics dust
16) Air, Smoke & Combustion Byproducts
PAHs, VOCs, particulates, dioxin byproducts
What / how formed:
Incomplete combustion generates complex hydrocarbon mixtures and fine particulates.
Endocrine relevance:
Can alter cortisol and thyroid signaling via inflammatory stress pathways; some compounds are endocrine-active and bioaccumulative.
Common exposure:
Wildfire smoke • Tobacco/vape aerosols • Indoor burning • Traffic pollution •Chemtrails • Marijuana
Side Bar: Cannabis Use and Endocrine Signaling in Midlife Women
Cannabis interacts directly with the hypothalamus and the feedback systems that regulate reproductive and stress hormones. In a woman who no longer menstruates, ovarian estrogen is low. Chronic THC exposure can dampen central signaling and alter cortisol output, especially with frequent use or consuming any THC-infused products. Because THC accumulates in fat tissue, repeated exposure creates sustained receptor stimulation rather than a brief effect. In a system that has already recalibrated to lower estrogen levels, additional disruption of the hypothalamic rhythm can worsen sleep disturbance, mood shifts, and metabolic instability rather than relieve them. And it has a cumulative effect; the longer you use it, the worse it gets. Passing out after eating a “gummy” doesn’t mean you are sleeping, just unaware of your wakefulness.
17) Food Service Packaging & Heat-Driven Migration (Exposure Amplifier)
PFAS, bisphenols, phthalates, styrene, microplastics
What / how formed:
Packaging is engineered for heat, grease resistance, and shelf stability; heat increases migration.
Endocrine relevance:
Hot fats and hot liquids accelerate the leaching of endocrine-active chemicals, increasing the internal dose.
Common exposure:
Takeout containers • Fast food wrappers • Coffee cups • Microwaved packaged foods • Hot soup in lined bowls
18) Water Contaminants & Treatment Byproducts
PFAS, perchlorate, heavy metals, pesticide runoff, disinfection byproducts
What / how formed:
Industrial runoff, agricultural runoff, and legacy contamination enter water; disinfection chemistry can create secondary byproducts.
Endocrine relevance:
The thyroid is especially sensitive. Chronic exposure contributes to hormone disruption.
Common exposure:
Tap water • Well water • Bottled water • Ice machines
19) “Wellness” Product Contaminants & Adulteration
Steroid/prohormone adulterants, estrogenic contaminants, heavy metal contamination (herbs), solvents/excipients
What / how formed:
Poor manufacturing controls, cross-contamination, or intentional performance product spiking.
Endocrine relevance:
Direct hormone receptor binding can suppress natural testosterone and disrupt menstrual cycling and fertility.
Common exposure:
Sports supplements • Testosterone boosters • “Detox” products • Imported herbs •Pre and Post workout drinks
20) Oncology & Radiation Exposure
Chemotherapy agents, ionizing radiation.
What / how formed:
Chemotherapy drugs are designed to disrupt DNA replication; radiation uses ionizing radiation to damage DNA.
Endocrine relevance:
It can damage ovaries/testes, disrupt thyroid tissue, and cause long-term fertility and hormone changes.
Common exposure:
Cancer treatment • Occupational radiation • Repeated medical imaging (context-dependent)
21) Salon, Nail & Hair Product Chemicals
Toluene, Formaldehyde, Formaldehyde-releasing resins, Dibutyl phthalate (DBP), Triphenyl phosphate (TPHP), Acrylates (EMA/MMA), Methacrylates, Ammonia, Hydrogen peroxide, Persulfates, Resorcinol, Paraphenylenediamine (PPD), Coal tar dyes
What / how formed:
Petrochemical-derived solvents, plasticizers, polymerizing monomers, oxidizers, and aromatic amines are used to harden nail coatings, bond artificial nails, permanently alter hair pigment, or bleach hair.
Endocrine relevance:
Plasticizers and organophosphate esters exhibit endocrine activity in laboratory studies. Metabolites of most nail polish additives have been detected immediately in the bloodstream directly after application, indicating systemic absorption. Repeated scalp exposure increases absorption potential. Chronic inhalation exposure in salons increases cumulative endocrine load.
Common exposure:
Nail polish • Gel nails • Acrylic/fake nails • Nail glue • Nail polish remover • Hair dye • Hair bleach • Root sprays • Dry shampoo • Hairspray • Scalp treatments • Salon fumes
22) Candles, Air Scenting & Indoor Fragrance Emissions
Synthetic fragrance blends, Phthalates (DEP), Paraffin wax (petroleum-derived), Benzene, Toluene, Formaldehyde (combustion byproducts), Synthetic musks, VOCs
What / how formed:
Paraffin wax is derived from petroleum refining. Fragrance blends are proprietary petrochemical mixtures. Combustion releases volatile organic compounds and particulates.
Endocrine relevance:
Inhaled fragrance plasticizers and combustion byproducts may contribute to an endocrine-active burden and oxidative stress, which can influence thyroid, cortisol, and reproductive hormone balance over time.
Common exposure:
Scented candles • Wax melts • Plug-in air fresheners • Room sprays • Car scent diffusers • Potpourri oils •Essential Oil Diffusers
Wake Up, You have been Played (Again)
So no, Virginia, there is no such thing as Santa Claus, and no, there is no such thing as menopause. You are TOXIC, and your toxic load has hit critical mass because you lost your primary detox pathway when you stopped menstruating. Now all the garbage you infuse yourself with is stuck in your body, looping around, accumulating in your burgeoning fat storage. You have become a garbage dump, a chemtrail, and a forever chemical wrapped up in yoga pants.
The Feedback Loop Consequence
As you can see, the endocrine system does not distinguish between estrogen produced by ovarian follicles and estrogenic activity introduced from outside compounds. Receptors respond to signaling. The hypothalamus and pituitary adjust output based on circulating levels and receptor activation.
If environmental exposures increase estrogenic signaling, the brain may reduce ovarian stimulation through negative feedback. If chronic stress elevates cortisol, reproductive signaling will be suppressed in favor of survival pathways. If adipose tissue increases aromatase conversion, estrogen levels rise independently of ovarian output. Over time, the body recalibrates.
When a woman presents with fluctuating cycles, mood changes, sleep disturbance, or weight gain, it is layered exposures, metabolic stress, and feedback adjustments influencing the system long before follicular depletion.
If the loop has already downregulated in response to external signaling, introducing additional exogenous estrogen further suppresses endogenous production. The body interprets circulating hormones only as it recognizes that hormone signaling occurs within a chemical and metabolic environment far more complex than that of anything seen before. So, adding pharma-made hormones or laughable “bioidenticals” to the already toxic soup? Out of the frying pan into the fire.
When talking about hormones, we can’t escape the alphabet cult. With the massive infusion of hormone disruptors, especially estrogen, we need to discuss the massive rise in those “identifying” as a letter and experiencing gender confusion and cross gender traits. And why the market is expanding into the pediatric population. Pause for a moment here. Do you think the convicted felons who make these drugs and market them to babies, children, and pubescent teens want anything beneficial for you? Again, they don’t make “good” drugs; they forgot about them. They just sell poison.
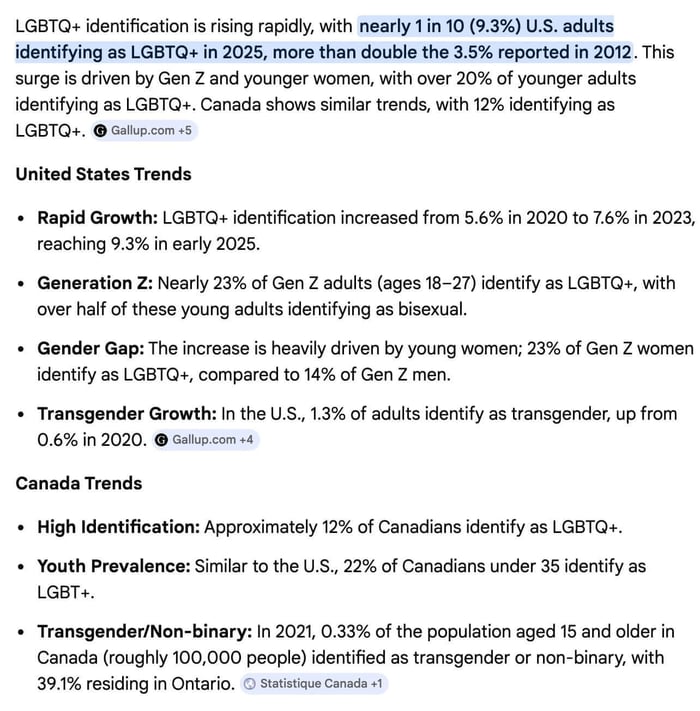
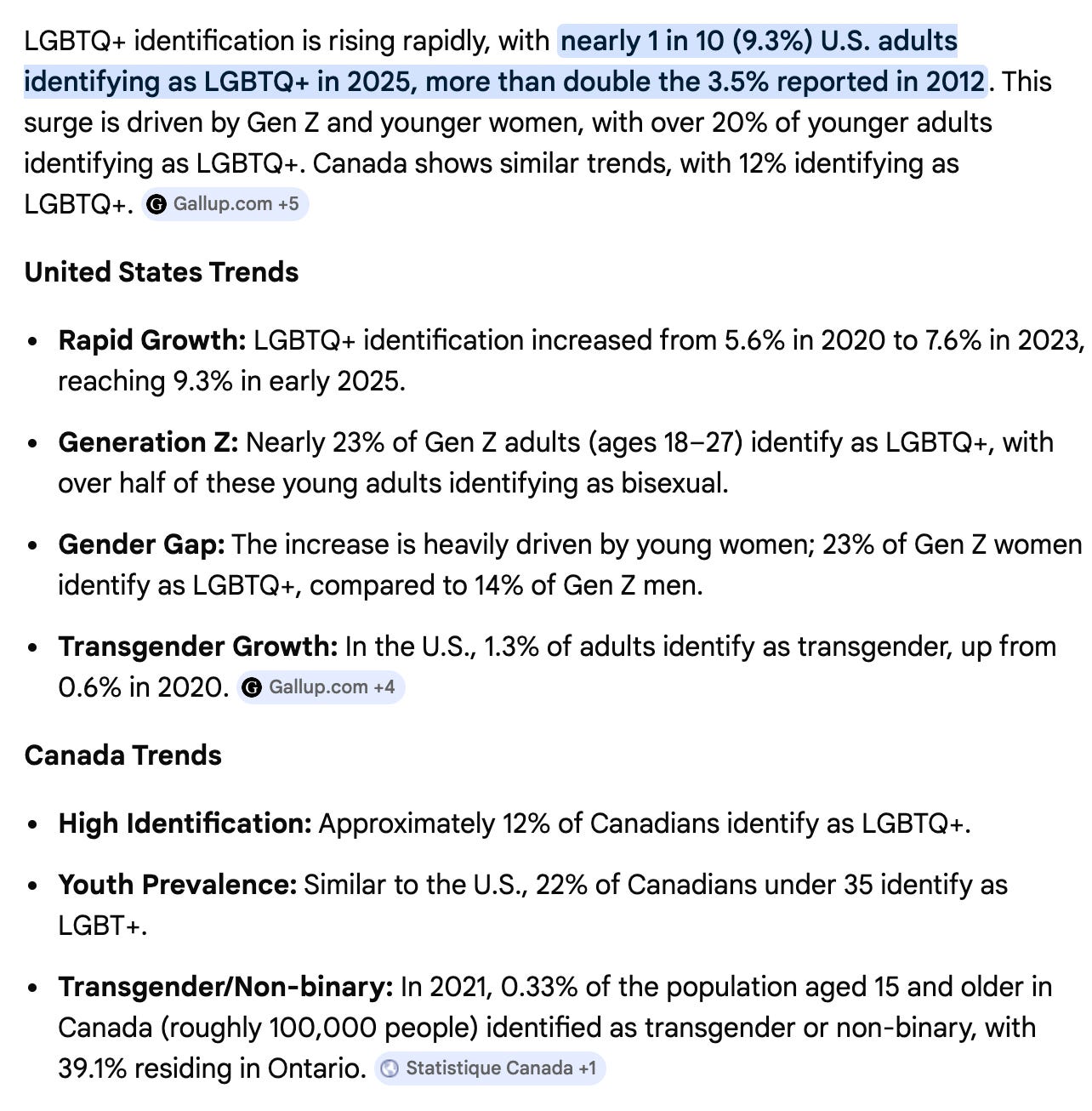

I have no idea how much infusing the population with massive amounts of Estrogen will do moving forward, but we can’t ignore numbers that have doubled. If there is anything more nefarious than just massive profits, it is the nature of the beast. What we do know is that this is on purpose and by design by the FDA, Big Food, Big Pharma, and the Medical Industrial Complex. No, they don’t have the “good” drugs, HRTs, and studies that help their customers. Only slowly making you worse, because it’s in their nature. They can’t deviate from profit, at your expense.
Conclusion
By now, the pattern should be clear. Menopause did not arrive as a biological observation. It was named, grouped, interpreted, and eventually monetized. Once synthetic estrogen became available, the transition from life phase to deficiency model was seamless. A natural recalibration of ovarian signaling was reframed as failure, and replacement became the solution.
At the same time, the modern hormonal environment changed dramatically. Chemical exposures multiplied 100x across food systems, textiles, cosmetics, pharmaceuticals, water, and indoor air. Stress physiology intensified. Sleep shortened. Adipose tissue increased. The endocrine system recalibrates in response to it all.
This is why dependence appears to develop. A woman may feel stable on estrogen and destabilized when she stops, not because her body was damaged, but because pharmacologic dosing replaced what her system was no longer producing at the same level. The therapy can conceal decline without reversing it. Once withdrawn, the underlying physiology remains, only slightly worse, depending on the duration of hormone use.
The important question is what sustained replacement does to clotting pathways, vascular tissue, breast stimulation, liver metabolism, adipose conversion, and central feedback regulation over the years of use. Immediate relief does not equal long-term neutrality.
That is where the final piece goes.
Article 4 will examine what long-term hormone replacement actually does inside the body, how delivery methods alter risk, how metabolism determines downstream effects, and what practical steps strengthen signaling without overriding it. It will include a printable solution framework that can be applied immediately.
Side Note
If reading this series has left you realizing how many layers are influencing your body, that reaction makes sense. Most women were never taught how the feedback loop works, how exposures accumulate, or how to reduce them without replacing one dependency with another. Once you see the system clearly, the next question is what to actually do with that information.
This will be the third consecutive year I have taught my 11-week course, and the majority of women from the first round returned because they found it practical, not theoretical. I teach it live. Each week includes one hour of structured teaching, followed by one hour of live questions or a hands-on demonstration, during which we walk through the food, household, and personal care shifts step by step. Over time, the group becomes a real community built on shared accountability and steady progress.
You leave with detailed guidance, sourcing strategies, recipes, and a structured plan to remove daily chemical exposure without becoming obsessive or overwhelmed. Most participants save at least $1,500 in the first year simply by eliminating poison products and unnecessary spending. I have also sourced and developed some of the cleanest products available, including select handmade items, so you do not have to sort through labels designed to mislead.
The goal is not short term detox enthusiasm. It is long term hormonal and financial resilience.
Article 4 examines what sustained hormone replacement actually does over time and what strengthens the system rather than suppressing it. That is where this series closes.
References
De Gardanne, C. P. L. (1821). De la ménopause, ou de l’âge critique des femmes. Paris: Méquignon-Marvis.
Wilson, R. A. (1966). Feminine forever. M. Evans & Company.
Watkins, E. S. (2007). The estrogen elixir: A history of hormone replacement therapy in America. Johns Hopkins University Press.
Writing Group for the Women’s Health Initiative Investigators. (2002). Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the Women’s Health Initiative randomized controlled trial. JAMA, 288(3), 321–333.
Gore, A. C., Chappell, V. A., Fenton, S. E., et al. (2015). EDC-2: The Endocrine Society’s second scientific statement on endocrine-disrupting chemicals. Endocrine Reviews, 36(6), E1–E150.
Diamanti-Kandarakis, E., Bourguignon, J. P., Giudice, L. C., et al. (2009). Endocrine-disrupting chemicals: An Endocrine Society scientific statement. Endocrine Reviews, 30(4), 293–342.
Rochester, J. R. (2013). Bisphenol A and human health: A review of the literature. Reproductive Toxicology, 42, 132–155.
Sunderland, E. M., Hu, X. C., Dassuncao, C., et al. (2019). A review of the pathways of human exposure to poly- and perfluoroalkyl substances (PFASs). Journal of Exposure Science & Environmental Epidemiology, 29(2), 131–147.
Hall, J. E. (2021). Guyton and Hall textbook of medical physiology (14th ed.). Elsevier.
Gorzalka, B. B., & Dang, S. S. (2012). The endocannabinoid system and gonadal hormones: Bidirectional interactions. Frontiers in Endocrinology, 3, 1–12.
Kinuta, K., Tanaka, H., Moriwake, T., Aya, K., Kato, S., & Seino, Y. (2000). Vitamin D is an important factor in estrogen biosynthesis of both female and male gonads. Endocrinology, 141(4), 1317–1324.
Gallup. (2023). LGBT identification in U.S. ticks up to 7.6%. Gallup News.