


The Precursor to Dementia
In the beginning of this series, we established that it is structured, cyclical, and actively regulated particularly REM sleep, which the brain defends, restores, and prioritizes even after deprivation. Dreaming is built into the system and as we have discovered, is anything but a passive state.
We then explored what happens when that carefully balanced sleep system is disrupted, not just in isolated moments, but repeatedly, through cycles of stimulation, suppression, and fragmentation. This ongoing interference leads not simply to less sleep, but to fundamentally altered biology: impaired memory, both short and long, cognitive slowing, and emotional instability. These are the kinds of changes that accumulate quietly but have dire consequences, showcasing the cumulative impact of disrupted sleep.
Despite these stacking disruptions, the response has not been to restore the system; instead, bandaid intervention are the obvious and ongoing approach.
Medications vitamins and supplement and shortcuts are introduced as solutions. However, these interventions do not recreate the sleep stages the brain strives to maintain. Instead, they induce sedation, shift timing signals, and blunt internal regulation. The result is an appearance of sleep, while the underlying structure remains altered, further compounding the mismatch between intended restoration and actual effects.
Since REM sleep is something the brain actively preserves, and its disruption carries measurable consequences, the question shifts: it is no longer just about whether sleep is being lost, but about how the nature of sleep itself is being changed and how that is changing the fabric of society. Not to be overly dramatic, but the sleep deprivation and loss of REM cycles in the majority of the population it becoming more apparent. I think you could see that in 2020 and beyond, those that have lost the ability to use logic and instead rely on television and black screen talking heads. And before you pat yourself on the back, if you took ivermectin, vitamins, supplements, coffee enemas, MMS, turpentine, methylene blue, magnesium, etc. etc. then you are just as blind and controlled as the vaxers. So lets stop blaming each other and look to the real culprit.
Sedation Masquerading as Sleep
Until now, we have mostly discussed disruptions caused by external inputs such as stimulants, light, environment, and behavior, which prevent the brain from entering sleep properly. Now, we turn to a deeper layer of interference: interventions that do not merely block sleep but actively replace its processes.
Drugs taken for anxiety, depression, and daily function do not stay isolated to daytime effects. They act on the same signaling systems the brain relies on at night, changing how sleep is organized at a level that is already sensitive to disruption.
The brain does not separate these functions. The signals that control mood and alertness during the day are the same ones that determine whether the brain can transition into REM at night. When those signals are artificially adjusted and held in place, the sleep state is dramatically altered for as long as the medications stay in the body. And some stay in for weeks, even months after the last dose was taken.
When you look at what is happening to sleep, REM suppression, constant fatigue, a brain that never fully recovers, it stops looking like an isolated issue and starts to look like part of something larger, more nefarious. As an aside, we keep looking to the elite, the World Economic Forum, the powers above us that we talk endlessly about. And why? We think if we discover who is behind this we can actually stop it? Consider this:
We don’t need lizard people, the 7 families and their “original bloodlines”, the cabal, the illuminati, the freemasons, vampires, fallen angels and other endless rabbit holes garnering our attention and endless debates and discussion. We simply need to look at the amount of money the corporations are collecting from making us fat, sick, weak, distracted, diseased, depressed, disillusioned, fearful, angry and addicted. There, mystery solved. Now turn off your screens and start creating solutions instead of kicking the can down the endless highway.
Below a picture is worth a thousand words. The next sequence sums up everything I know about the medical system without saying a single word.






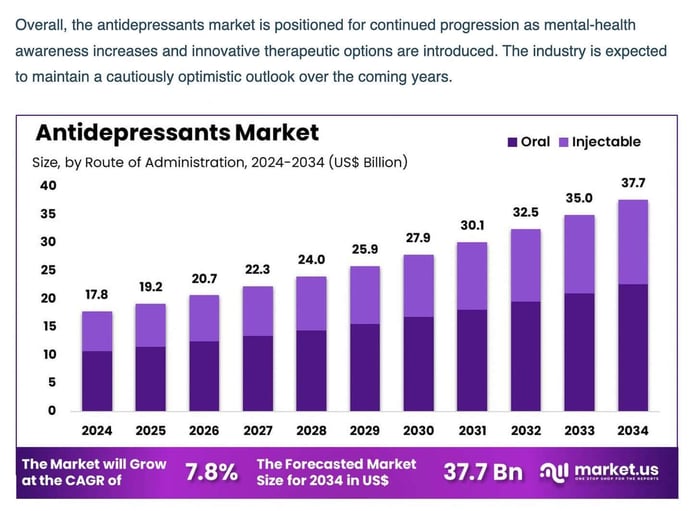
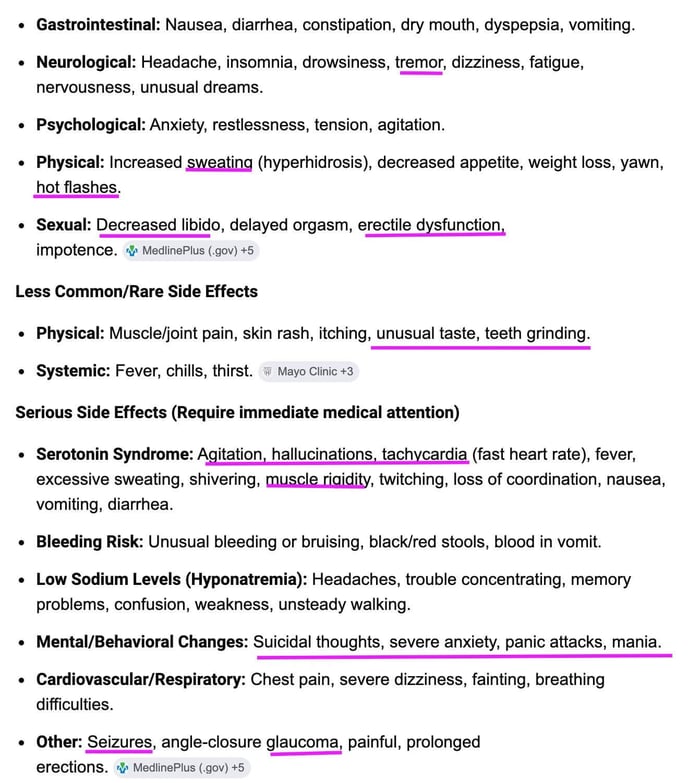
Antidepressants are one of the clearest examples. SSRIs, SNRIs, and MAOIs increase serotonin and often norepinephrine. By the way, even their corporate-funded research shows that these “neurotransmitters” have nothing to do with depression and that antidepressants don’t work, but as you can see, that hasn’t even put a dent in the 18 billion dollar industry, set to double by 2030. We learned in my college psych class the 1/3 rule in psychology. 1/3 gets better, 1/3 doesn’t change, 1/3 gets worse, no matter what “therapy” such as antidepressants, psychoanalysis, or no treatment is given to the subject. Yes, the field of psychology is filled with just as much bullsh#$ as the medical system but this has made zero impact on the pharmaceutical machine. Look at the projected rise in the antidepressant market. 17.8 Billion, expected to more double by 2034. This is the real fuel for the matrix money siphoning machine.
Back to neurotransmitters: these are wake-promoting signals. They are supposed to drop at night to allow REM sleep to begin. When they stay elevated through synthetic drugs, the transition is blocked. REM is pushed to the next night, or suppressed altogether. Sleep continues, but the REM phase the brain is actively trying to reach is decreased or deleted altogether.
Antidepressants also stay in the system far longer than most people realize. These drugs have long half-lives, meaning they stay in the bloodstream and tissues and continue to affect the brain well beyond the time they are taken. The signals they alter are not briefly adjusted and then cleared. They are sustained for long periods of time.
Fluoxetine, commonly known as Prozac, is one of the clearest examples. It can remain active in the body for weeks, with metabolites that extend its effects even further. In practice, this means the brain is continuously exposed to elevated serotonin signaling, day and night, without a true off period. There is no window for the system to fully return to baseline and complete normal REM cycling.
This is not a single night of disruption. It is ongoing. If the brain requires a reduction in these signals to enter REM, and those signals are being maintained around the clock, then REM is not just delayed. It is repeatedly restricted.
Even after stopping the medication, the effects do not end immediately. The system takes time to recalibrate. During that period, sleep remains altered, and REM remains unstable as the brain attempts to regain its normal rhythm.
Let’s add in teenagers taking antidepressants and their increased need for more sleep. Suppressing the REM cycles could be an underlying cause for suicidality, homicidality, grandiose and or delusional thinking. This is also a listed side effect on antidepressant medication. This is for Prozac.
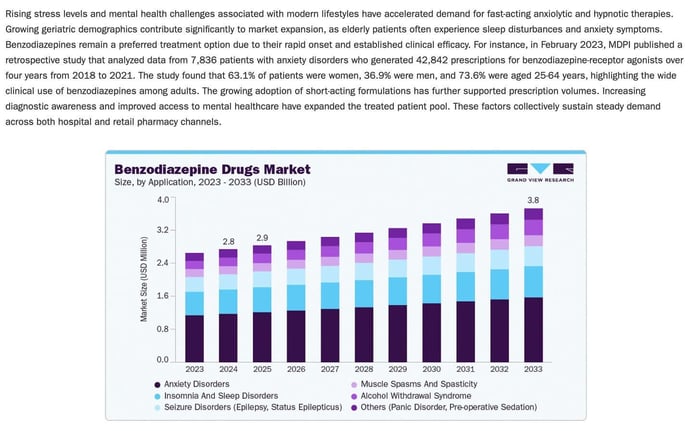
Benzodiazepines move in the opposite direction but create the same outcome. They suppress brain activity broadly, making it easier to fall asleep and remain asleep. But sleep is not meant to be a flat state. It is supposed to move. When the system is overly dampened, the normal rise and fall between stages is lost. REM becomes shorter, unstable, and more easily interrupted. Bottom line? The REM you are getting is just as synthetic as the drug. It doesn’t count.
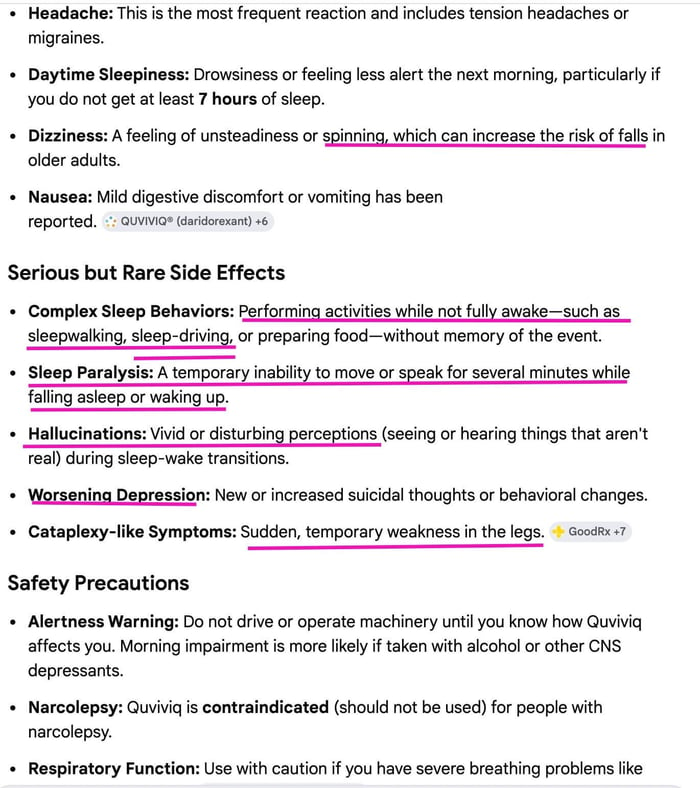
Sleep medications known as hypnotics such as zolpidem, eszopiclone, and zaleplon are often presented as more precise. They are marketed as helping the brain “sleep” without the broader effects of older drugs. But they still act by forcing the brain into unconsciousness. They do not recreate the natural pattern. They override it. REM sleep is obliterated for the length of time the drugs are taken. Hence the REM rebound and the horrific side effect profile of the drugs. The hallucinations are occurring because REM is not. Again, the brain needs REM like the lungs need air.
Across all of these, the pattern is the same. The person is asleep, but the brain is not cycling the way it is designed to. The signals that allow REM to emerge are either held too high or flattened too broadly, and the transition into that state becomes unstable.
When REM is removed or even just reduced, the brain does not ignore it. It keeps track. It builds pressure to recover what was missed. When that pressure finally releases, REM returns earlier, stronger, and less controlled. Dreams intensify. Sleep becomes uneven. The system is trying to correct for something that has been repeatedly blocked.
That does not happen with optional things. We need air, sunlight, water, food, and REM sleep.
The brain does not fight to recover from light sleep. It does not compensate for drifting in and out. It compensates for REM. When this pattern repeats night after night, the brain is no longer completing its normal cycle. It is operating under interference. Sleep is happening, but recovery is not happening in full.
But What About the Herbs and Supplements?
So what are we left with? Supplements that everyone loves to tell you to take, as though they have any idea what they are talking about. They are simply repeating what they heard like a good parrot. Remember, foxglove is Digoxin, not a synthetic take, but crushed foxglove plant makes one of the most powerful and dangerous cardiac drugs on the market. You repeating the idea that Rockefeller took over the “good” side of medicine-herbs, plants, roots, vitamins-is dead wrong. He played both sides. And Digoxin tells you they can patent a plant, so stop repeating what they want you to. While natural, wild plants cannot be patented, they can be protected through specific types of intellectual property if they are modified, “discovered in a cultivated state”, and asexually reproduced. So, yes the herbs can damage you just as much as the drugs, and some are the same.
Valerian root and other “natural” sleep remedies that are treated differently from drugs, but they act on the same systems and produce many of the same effects. People report headaches, dizziness, mental fog, gastrointestinal issues, and inconsistent sleep, including restlessness, insomnia, and vivid dreams. Same side effects as sleeping pills.
At higher doses, they can cause next-day grogginess, and in some cases, more serious effects such as liver strain, heart palpitations, and withdrawal symptoms after prolonged use. They also dangerously interact with alcohol, sedatives, and other medications, amplifying suppression of the nervous system. The label may be different, but the mechanism is not. These compounds still push the brain into sedation rather than allowing it to move through its natural sleep cycle, leading to the same outcome, altered and reduced, unstable REM sleep.
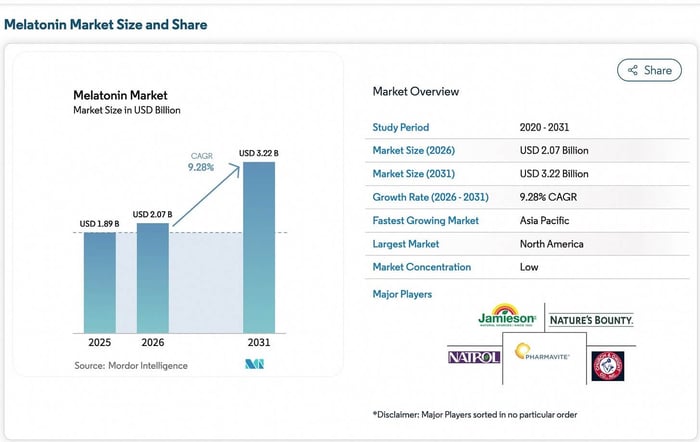
But what about everyone’s favorite all natural from the good guys melatonin?
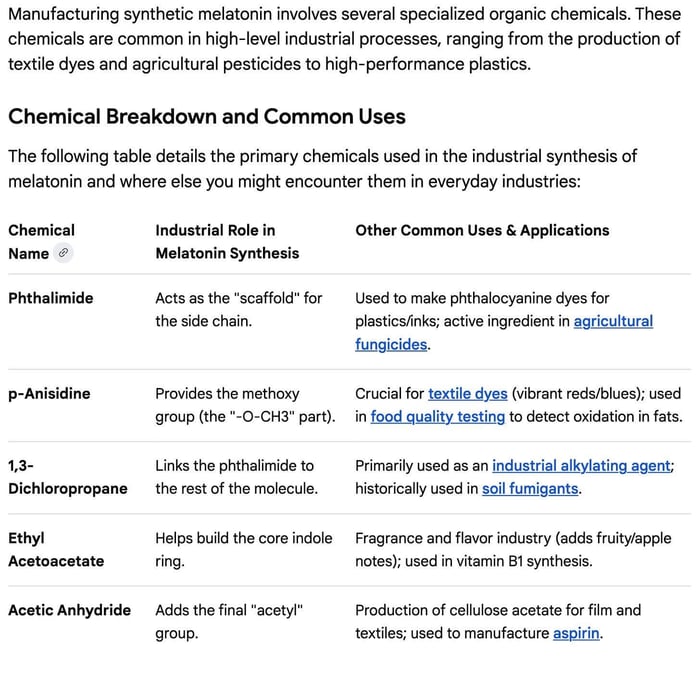
Melatonin is made from Feces

Melatonin is the one people trust. After everything else fails, after the stimulants, the late nights, the medications—this is what people reach for to “fix” sleep. It’s sold as natural, something your body already makes, something safe enough to take every night without question. But nothing about how it is used reflects how it actually works.
This anything but natural hormone they tell us regulates sleep, is produced industrially using a hybrid system that combines human feces and chemistry, just like vitamin B12. The process begins with E. coli bacteria obtained directly from human feces, which act like microscopic factories. (But this is the “good” E. coli, not the “bad” E. coli that causes outbreaks in restaurants and at picnics and makes people sick.) Well, it is obviously just a cover story for the chemicals they use to poison food, but E. coli is still disgusting and should be off the menu, in my opinion. These bacteria 100x when they are fed simple, inexpensive materials such as glucose, along with nitrogen sources such as ammonium salts, and trace metals such as iron and zinc that support enzyme activity. What a great thing to take every night.
Melatonin and E-Coli Poopcakes?
Melatonin in the body is not a sleeping pill. It is a signal. It rises in response to darkness, signaling to the brain that night has begun. It does not create sleep. It does not control the stages. It does not force REM. The brain still has to move through that process on its own. What is being taken externally is something very different in how it is produced and how it is used.
They will tell you that they just use the original crap from some dude and grow it like sourdough, but tell me this. Would you eat pancakes from someone using decades old e-coli poop kept alive with sugar? I didn’t think so.
Once production is complete, the melatonin is not isolated. It exists inside a dense mixture of bacterial material, proteins, and metabolic waste. From there the mixture is broken down, separated, and refined using chemicals listed below, adjusting pH with strong acids and bases, extracting the compound, and making a new chemical laden soup (what they call isolating) using methods such as chromatography.
Further steps may be used to finalize the molecule using common industrial reagents used in chemical manufacturing. The end result is a chemical Frankenstein compound that roughly matches the structure of endogenous melatonin.
If the system is already disrupted, adding melatonin does not repair or rebuild it. It simply masks it. It shifts one signal while everything else remains unchanged. Sleep may come more easily. But the structure underneath is not restored. REM is not guaranteed. The brain is still working around interference. This is the same pattern seen everywhere else. The system adapts, but it does not recover.
THE CYCLE OF INTERVENTION
This is not one problem, it is a loop. Sleep gets disrupted, REM is shortened or delayed, and the next day you feel it—fatigue, brain fog, slower thinking. Instead of fixing what caused it, you push through it. Caffeine, nicotine, anything to stay functional. Those signals don’t go away, they just get carried into the night, where sleep becomes harder or more fragmented. So you add something else—medications, supplements, something to knock you out or shift the timing. You may sleep longer, but the structure is still off. REM stays unstable because the brain never gets back to baseline. Then the next day you feel it again, and the cycle repeats. More stimulation, more suppression, less recovery. Over time, this becomes normal. Sleep starts to depend on intervention, but nothing being added actually restores the system. It just keeps you going without ever fully repairing what’s being lost.
A typical version of this looks familiar. A couple of glasses of wine at night to relax, take the edge off, slow things down. Sleep comes easier, but alcohol suppresses REM early in the night and fragments it later. It is just passing out and not being aware you are not sleeping properly. The brain does not complete its cycle, so the next day starts with fatigue. Coffee picks up the slack, maybe more than one. The signals get pushed forward again. Night comes, and instead of real sleep pressure, there is stimulation still in the system, so melatonin gets added to force the timing. Sleep happens, but the structure is still off. REM is delayed, uneven, or reduced, and the same pattern carries into the next day. Nothing in that sequence restores the system. Each step compensates for the last one while keeping the cycle in place. Repeat this pattern for a few years or decades and you are headed for disaster.
Disrupted REM, Disrupted Memory
At this stage, the effect is no longer limited to how someone feels the next day. The changes begin to show up in how the brain stores and maintains information.
REM sleep plays a central role in memory consolidation. During this phase, the brain takes newly formed, unstable memories and integrates them into longer-term storage. Emotional experiences are processed, and their intensity is reduced so they can be retained without overwhelming the system. At the same time, the brain increases clearance of metabolic waste, including proteins such as amyloid-beta and tau, which are associated with neurodegenerative disease when they accumulate.
When REM sleep is reduced or repeatedly disrupted, these processes do not occur in full. Memory consolidation becomes incomplete. Information that should be stabilized remains fragile or is lost. Emotional memories are not processed in the same way, leading to stronger stress responses and poorer regulation. Chronic disruption begins to produce measurable, observable changes in the brain.
Reduced REM sleep has been associated with lower levels of brain-derived neurotrophic factor, which supports neuron survival and plasticity, and higher levels of cortisol, which can physically damage structures involved in memory formation, particularly the hippocampus. Over time, this creates conditions where new memories are harder to form and existing ones are less stable. Also known as dementia and Alzheimers. Add in lower cholesterol, secosteriod hormones like HRT, Vitamin D3 and you have a perfect storm for a fate worse than death.
There is also evidence that disrupted sleep contributes to structural changes. Damage to small blood vessels in the brain and changes in white matter have been observed in individuals with long-term sleep disruption, particularly when REM is consistently affected. These are not functional changes alone. They reflect physical alteration of brain tissue.
The clearance process is also affected. When REM sleep is insufficient, the brain’s ability to remove metabolic waste is reduced. Proteins that are normally cleared begin to accumulate. Over time, this is one of the mechanisms linked to neurodegenerative conditions.
These changes do not appear immediately, and they are not always obvious at first. Early on, they present as forgetfulness, slower recall, reduced focus. With continued disruption, the deficits become more persistent. Crying jags, angry outbursts, constantly losing your keys and wallet, losing paperwork, forgetting appointments and anxiety are warning signs.
Short-term sleep loss can often be recovered from when normal sleep resumes. Chronic disruption is different. When the system is altered over long periods, recovery becomes incomplete, and some deficits may persist. At that point, the issue is no longer fatigue or poor sleep quality. It is a permanent change in how the brain maintains memory, processes information, and preserves its own structure over time.
Conclusion
At some point, this stops being about sleep and starts being about what the brain is no longer able to do.
When REM is consistently disrupted, the loss does not stay contained to the night. The brain is still running, but it is not completing the phase it depends on to maintain itself. Memory is not stabilized the same way. Emotional experiences are not processed and resolved. Signals that should be cleared remain active longer than they should.
Proteins that are normally cleared begin to build. Regions responsible for memory and learning become more vulnerable. The same patterns seen in dementia and Alzheimer’s disease begin to take shape, not as a sudden event, but as a gradual failure of maintenance. What looks like aging or decline is often the result of a system that has not been allowed to fully reset.
The effects do not stop there. When emotional processing remains incomplete, mood becomes less stable. When neural signaling becomes less efficient, motor function begins to change. This can look like Parkinson’s disease, Myasthenia gravis, Guillain-Barré syndrome, Amyotrophic lateral sclerosis, Multiple sclerosis, Huntington’s disease, Peripheral neuropathy, Spinal muscular atrophy, Muscular dystrophy, Charcot-Marie-Tooth disease, Progressive supranuclear palsy, Corticobasal degeneration, Essential tremors etc. All of the out of nowhere disease people think are just bad luck or bad genes.
Solutions
The problem is not that sleep is failing. It is that the conditions required for it have been replaced, step by step, with things that prevent it from ever completing. What restores REM sleep is not anything close to what people have been told.
It is not found in a bottle, and it does not come from increasing control over the system. The methods are simple, but they are not what you would expect, and they are not what you would hear in any medical setting. Some of them will sound wrong at first. Because once you understand what REM actually requires, it becomes clear why nearly everything people are doing to fix their sleep is keeping it from happening. And why removing those inputs changes everything.
References
Cajochen, C., Frey, S., Anders, D., Späti, J., Bues, M., Pross, A., Mager, R., Wirz-Justice, A., & Stefani, O. (2011). Evening exposure to a light-emitting diode (LED)-backlit computer screen affects circadian physiology and cognitive performance. Journal of Applied Physiology, 110(5), 1432–1438.
Chang, A. M., Aeschbach, D., Duffy, J. F., & Czeisler, C. A. (2015). Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proceedings of the National Academy of Sciences, 112(4), 1232–1237.
Drake, C., Roehrs, T., Shambroom, J., & Roth, T. (2013). Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. Journal of Clinical Sleep Medicine, 9(11), 1195–1200.
Hale, L., & Guan, S. (2015). Screen time and sleep among school-aged children and adolescents: A systematic review. Sleep Medicine Reviews, 21, 50–58.
Jaehne, A., Unbehaun, T., Feige, B., Lutz, U. C., Batra, A., & Riemann, D. (2009). How smoking affects sleep: A polysomnographical analysis. Sleep Medicine, 10(4), 490–495.
Ohayon, M. M., Carskadon, M. A., Guilleminault, C., & Vitiello, M. V. (2004). Meta-analysis of quantitative sleep parameters from childhood to old age. Sleep, 27(7), 1255–1273.
Wright, K. P., Jr., Hughes, R. J., Kronauer, R. E., Dijk, D. J., & Czeisler, C. A. (2001). Intrinsic near-24-hour pacemaker period determines limits of circadian entrainment. Proceedings of the National Academy of Sciences, 98(24), 14027–14032.
Xie, L., Kang, H., Xu, Q., Chen, M. J., Liao, Y., Thiyagarajan, M., O’Donnell, J., Christensen, D. J., Nicholson, C., Iliff, J. J., Takano, T., & Nedergaard, M. (2013). Sleep drives metabolite clearance from the adult brain. Science, 342(6156), 373–377.
Walker, M. P. (2017). Why we sleep: Unlocking the power of sleep and dreams. Scribner.
Rasch, B., & Born, J. (2013). About sleep’s role in memory. Physiological Reviews, 93(2), 681–766.
Palagini, L., Biber, K., & Riemann, D. (2013). The genetics of insomnia—evidence for epigenetic mechanisms? Sleep Medicine Reviews, 18(3), 225–235.
Meerlo, P., Havekes, R., & Steiger, A. (2015). Chronically restricted or disrupted sleep as a causal factor in the development of depression. Current Topics in Behavioral Neurosciences, 25, 459–481.
Winer, J. R., Mander, B. A., Helfrich, R. F., Maass, A., Harrison, T. M., Baker, S. L., Knight, R. T., & Walker, M. P. (2019). Sleep as a potential biomarker of tau and β-amyloid burden in the human brain. Journal of Neuroscience, 39(32), 6315–6324.



![Magnesium Vs. Zinc The Battle Royale That Ends the Debate [By Medicine Girl]](https://dropinblog.net/cdn-cgi/image/fit=scale-down,format=auto,width=700/34264201/files/featured/94577ece-6b84-4d7c-b622-6e764231d715.png)

![The Great Vitamin Liars Vitamins [Part 1 By Medicine Girl]](https://dropinblog.net/cdn-cgi/image/fit=scale-down,format=auto,width=700/34264201/files/featured/0c2c0703-aac4-4a09-8bbb-aa55f98bf33e.png)

