![The Great Vitamin Liars Vitamins [Part 1 By Medicine Girl]](https://dropinblog.net/cdn-cgi/image/fit=scale-down,format=auto,width=700/34264201/files/featured/0c2c0703-aac4-4a09-8bbb-aa55f98bf33e.png)

Why This Series Matters Now
This series examines the birth of the vitamin industry, how it began, how it expanded, and why it matters more today than at any point in history. The vitamin and supplement industry is booming. And it is the pharmaceutical industry. No two ways about it. They invented vitamins and supplements. They own and operate the companies. They make them in the EXACT same way as pharmaceuticals. Yet you have trouble distinguishing fact from fiction because your Con19 heroes are telling you these poisons are the good ones, so you accept on blind faith. Which is more poignant than ever as we will discover. It isn’t just ivermectin that causes hair and vision loss as I will point out later in this series on the B Vitamins and the birth of the biggest and most destructive industry since vaccines.

The common story is familiar. Deficiency diseases were identified, nutrients were produced in a lab with toxic CHEAP chemicals, isolated, and modern-for-sale science scammers stepped in to solve the problem. Vitamins became essential, fortification became policy, and supplementation became routine. The borrowed narrative from the vaccine story presents this progression as one of modern medicine’s great successes.
Of course, this version of events leaves out a little something I like to call the truth. Rare when you look at the lies research grifters use from the pHARMaceutical industry to write articles about the benefits of magnesium, while profiting from and selling magnesium. The fact that I even need to point that out baffles me. You can see it with the vaxers like Fuci, but not the same villains selling D-Con D3 and Methylene Blue. They are all about the benjamins, nothing more, nothing less. And they couldn't care less if they poison you or your family in the process. As long as the money keeps rolling in, they align with the paid-for science that lines their pockets.
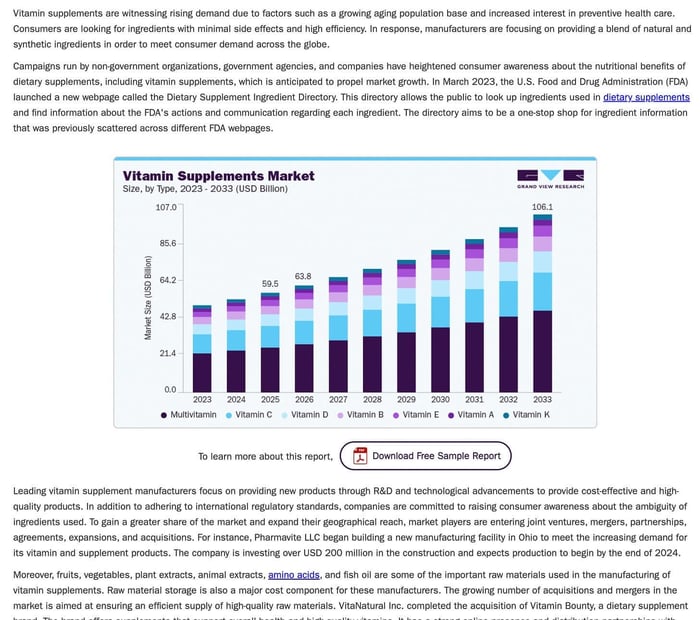
The purpose of this series is not only to dismiss deficiency diseases outright, but also to show how they were defined, how their causes were narrowed, and how those conclusions have built an industry that now operates at a global scale of 100 billion. The focus is on what was emphasized, what was ignored, and what changed at the exact moment these explanations became dominant. Of course, it goes without saying that the pharmaceutical giants that run the vitamin show have an endless budget to buy university studies, second-rate influencers, and wolves in sheep’s clothing puppets.

This matters because the system built on those early lies and assumptions is still shaping public health today, and the results are increasingly difficult to reconcile.
In the United States, thousands of chemical substances are permitted in the food and beverage supply, many under regulatory frameworks that rely heavily on industry-provided safety data. Industrial agriculture involves the routine use of tons of chemical inputs at multiple stages of production, including compounds used to accelerate crop desiccation prior to harvest. Food is chemicalized, processed, stabilized, preserved, and fortified on a scale that did not exist a century ago.
At the same time, the United States leads the world in the consumption of dietary supplements and pharmaceutical drugs, yet continues to experience rising pandemic rates of obesity, metabolic dysfunction, and chronic illness across both adults and children. Indicators associated with long-term population health, including massive fertility declines and maternal outcomes, while infant mortality remains elevated relative to even third-world nations.
The Crisis of Listening to Influencers
Independent investigations, such as those, have highlighted what is often referred to as a “crisis of science,” not a single failure, but a convergence of systemic pressures that shape how research is conducted, published, and interpreted. These include well-documented problems such as reproducibility failures, statistical manipulation through practices like p-hacking, publication bias favoring positive results, and the influence of funding sources on research direction and outcomes.
Even within mainstream academia, concerns have been raised that a significant portion of published research findings may not be reliable, particularly in fields where studies are small, variables are numerous, and incentives reward novel or attention-grabbing conclusions over null results. In such an environment, what is presented as settled science may, in reality, reflect a combination of methodological constraints, selective reporting, and institutional bias.
This basically invalidates science as a method, not to mention completely outs the assumption that consensus automatically reflects truth, especially since research intersects with commercial or policy interests.
The global market for fortified foods and vitamin supplementation has grown into a massive economic sector, valued in the hundreds of billions and projected to expand significantly in the coming years. What began as a targeted intervention has evolved into a system in which nutritional adequacy is increasingly defined by the presence or absence of manufactured compounds added back into processed food.
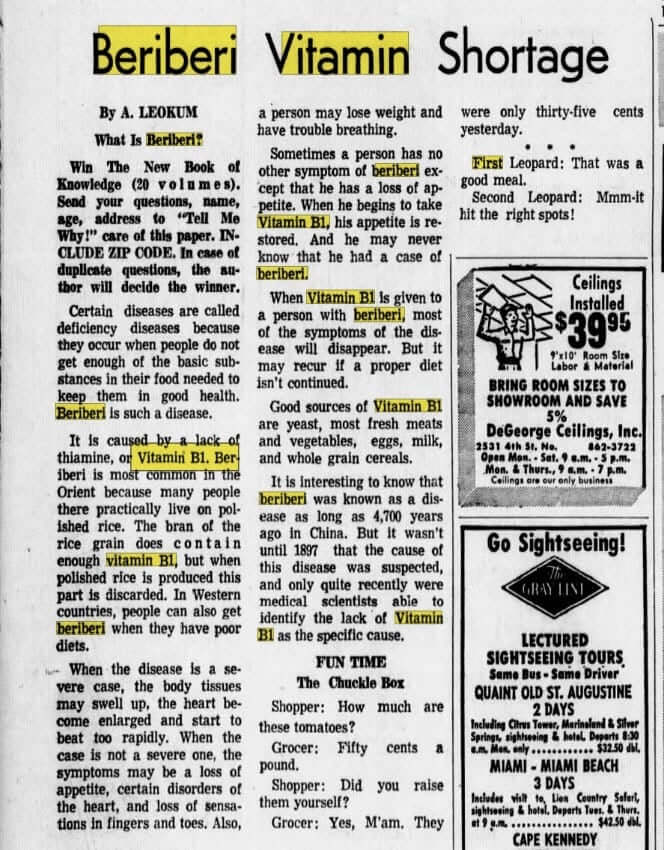
The early identification of conditions such as Beriberi led to the isolation of Thiamine and, from there, to the development of a model that would be applied repeatedly to other diseases and nutrients. What began as an attempt to explain a specific set of symptoms evolved into a broader system that redefined food, health, and deficiency itself.
The question is how a complex set of environmental, dietary, and industrial changes was reduced to a series of isolated variables, and how that reduction became the foundation of an industry that continues to expand, even as overall health outcomes decline.
Remember That Time When “Deficiency” Became a Market
As the manufactured and made-up beriberi crisis intensified between roughly 1880 and the 1930s, what unfolded on the ground did not look like a clean, single-cause disease but instead a single-cause solution. Governments, trade organizations, and colonial administrations were not responding to an abstract nutritional theory; they were reacting to real-world breakdowns in food stability, storage, and distribution that were producing illness on a scale that could not be ignored.
When something that has worked for generations suddenly starts failing, you don’t blame the thing itself. You look at what changed. And during that period, almost everything changed at once.
Never Let a Crisis Go to Waste

The Rice Riots brought millions into the streets over shortages, speculation, and instability in the food supply. Within three years, the government passed the Rice Law of 1921, effectively taking control of pricing, storage, and distribution. This was not just about economics. Officials were increasingly concerned with the condition of the rice itself, how it was stored, how long it sat, and what happened to it over time. Translation: they couldn’t poison the food supply if they didn’t have direct control over it. Moisture, spoilage, and degradation were suddenly being treated as serious risks. In commercial settings, cooked rice was often required to be discarded within a short window, sometimes within a day, because it was now believed that deterioration could produce harmful effects. Lol, they have no shame. The only thing worse than these mafia tactics? People buy them hook, line, and sinker.
By 1918, the situation surrounding rice in Japan had reached a breaking point that had nothing to do with a simple nutritional story. These Rice Riots involved over a million people across nearly 500 locations, with protests erupting from small fishing villages like Uozu and spreading rapidly through cities, mining towns, and agricultural regions in 42 of 47 prefectures. Prices had more than doubled in the wake of World War I, driven by speculation, hoarding, and government demand to supply troops during the Siberian Intervention, while wages for ordinary families remained stagnant. History sure has a way of repeating itself. Women in coastal communities were among the first to act, physically blocking rice shipments from leaving their towns, and what followed was not a symbolic protest but a direct confrontation, merchant shops destroyed, police stations attacked, and the military ultimately deployed to suppress the unrest. Over 25,000 people were arrested, thousands were convicted, and the crisis forced the resignation of Prime Minister Terauchi Masatake.
That is the environment in which the beriberi narrative was created, amid a full-scale, deliberately engineered breakdown of the food system. Rice was no longer a stable, locally managed staple. It becomes a controlled, traded, and manipulated commodity, subject to storage issues, transport delays, degradation, and contamination. Populations were being pushed onto simplified diets under unstable, deteriorating conditions. Yet within that complexity, the explanation that took hold reduced the problem to a single missing factor, eventually identified as Thiamine.
When everything changes at once, economics, storage, distribution, and food quality, you don’t isolate one variable and call it a solution, unless that was the plan from the beginning. And of course, that is exactly what happened. The broader crisis created the conditions, the symptoms appeared within that system, and the explanation narrowed at the exact moment when a single, controllable solution became possible.
And that solution did not remain theoretical for long. Within a matter of years, thiamine was isolated, structurally characterized, and synthesized, with companies such as Merck & Co. quickly moving into production. The pharma giants know a goldmine when they see it. What had emerged from a period of instability and system-wide stress was now reframed as a problem that could be corrected with a single manufactured input. The complexity of the crisis remained in the background, while the solution moved to the forefront—repeatable, scalable, and ready to be inserted back into the very system that had changed in the first place. Not to be overly repetitive, but this is the identical situation that occurred with every other single pandemic, including ol’ lucky number con 19.
Similar concerns were emerging elsewhere under a different language. In 1906, the United States passed the Pure Food and Drug Act in response to widespread adulteration in the food supply. Substances used to alter appearance or extend shelf life were being added without oversight, and rice, already a globally traded commodity, was part of that system. In U.S.-controlled territories such as the Philippines, beriberi was observed in institutional populations fed tightly controlled diets.
By the early twentieth century, rice had become a fully industrialized global commodity, moving through export systems in Burma, Thailand, Vietnam, and beyond. Yes, we are a one-world government and have been for quite some time. Trade organizations such as the London Corn Trade Association enforced strict standards, and shipments that arrived discolored or degraded, especially “yellow rice,” were rejected or penalized. Merchants could be blacklisted from entire markets if they were associated with contaminated grain. Governments imposed export bans when supplies were considered unsafe. None of that happens unless there is a consistent, observed problem. And we had a consistently observed and createdproblem.
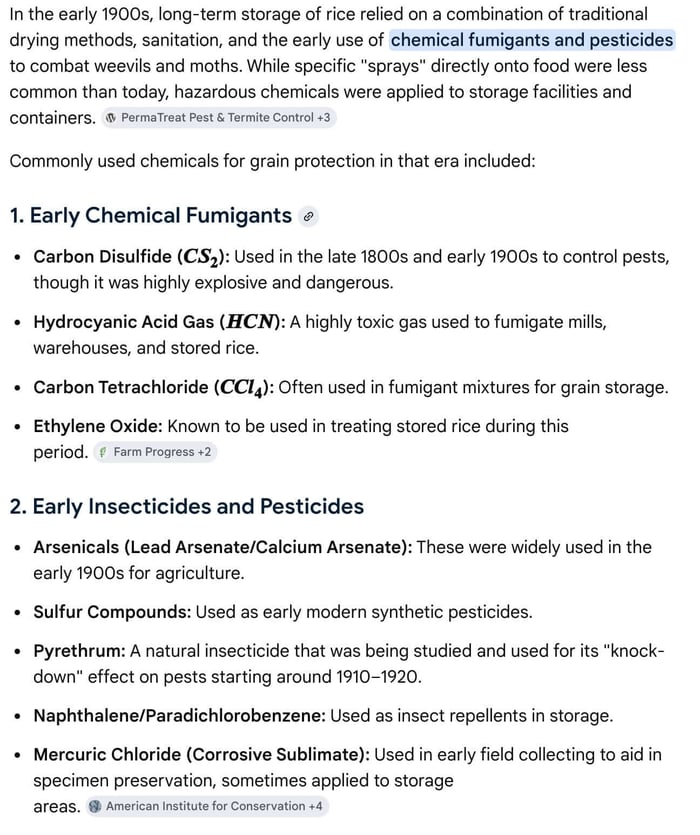
As scientific investigation progressed through the 1910s, 1920s, and into the 1930s, researchers began identifying “toxins” that developed on stored rice under humid conditions. They also used the chemicals listed above. It is not the mold causing the problems; it is the chemicals they use to store the grains. They produced compounds, later including toxins such as citreoviridin, that could induce neurological and cardiac symptoms in exposed populations. The problem is that those symptoms overlapped almost exactly with what had been labeled as beriberi. Oops, you did it again, Big Pharma!
Now you have a situation where two different pathways, nutritional depletion and toxic exposure, can produce nearly identical outcomes in the body. And they are both present at the same time within the same food system, under rapidly changing conditions driven by industrialization, storage practices, and global trade.
What followed was not a full resolution of that complexity, but a narrowing of it. The deficiency model, focused on the absence of something NEVER found in nature, Thiamine offered a convenient, profitable explanation that others did not. It was measurable. It could be mass-produced under controlled conditions. It could be corrected with a single intervention. It turned a system-level problem into a single-variable equation. $$$
At that exact moment, industrial chemistry was advancing rapidly. Pharmaceutical manufacturers, Merck & Co. and its European counterparts, were developing the ability to create and synthesize cheap compounds at scale. What had once existed as part of a complex, inseparable food system could now be broken apart, named, reproduced, and sold.
The shift was immediate and profound. A disease framed as the result of a missing dietary factor no longer requires rebuilding food systems or addressing environmental conditions. That is key. The problem and its solution lie entirely within corporate and governmental controls. Tablets, powders, and eventually fortified foods replaced the need to return to the system as a whole. The problem had been solidified into something that could be manufactured.
![]()
From there, scaling was inevitable. Populations in Asia, particularly those relying heavily on rice in institutional, military, or colonial settings, became the central focus of early deficiency lies and interventions. If disease could be attributed to the absence of a single compound, and that cheap-to-make compound could be produced in bulk, then the solution could be standardized and applied across entire populations. Diet became an input-output equation: deficiency identified, compound supplied, outcome corrected. Virus detected, vaccine injected, outcome corrected.
That model did not require restoring traditional dietary diversity. It did not require solving storage problems, contamination risks, or environmental degradation. It required production, distribution, and compliance.
And once it worked, even partially, it became a public fact as infrastructure.
Over time, this approach expanded beyond thiamine. The same framework was applied to other nutrients: identify a deficiency, isolate the compound, manufacture it, and integrate it into the food supply. What began as an intervention became a system. Food was no longer evaluated as a complete structure, but as a delivery vehicle for specific compounds, regardless of how those compounds were introduced.
The Dissolution of Science
This is where the crisis of science enters the picture as a recognition of how scientific conclusions are shaped under pressure. In any complex system with multiple variables, the explanation that survives is not always the one that accounts for everything. It is the one that can be tested, reproduced, funded, and scaled. Deficiency can be blamed on the toxic chemicals, and of course, it will meet those criteria.
The issue is not whether a deficiency exists. It doesn’t.
What followed from that foundation was not just the acceptance of a model, but the rapid expansion of an industry built around it. Once Thiamine could be sold as something more than a chemistry experiment and mass-produced, so now it could be distributed and applied consistently. The answer, by the 1920s and 1930s, was clear: at scale, and everywhere.
Industrial chemistry had reached a point where compounds could be synthesized in controlled environments using standardized processes. Pharmaceutical manufacturers, including Merck & Co. and others operating in Europe and the United States, were no longer limited to extracting substances from natural sources. They could produce them independently, in bulk, and with a level of consistency that made integration into food systems not only possible but efficient. What had once existed within a complex nutritional environment was now treated as a standalone input, something that could be inserted back into the system after processing had stripped it away.
At that point, the logic becomes difficult to ignore. If a disease is defined by the absence of a compound, and that compound never existed in nature, and the compound can be manufactured cheaply at scale, then the solution is no longer constrained by agriculture, geography, or traditional diet. It becomes a matter of production and distribution. The complexity of food is replaced with a repeatable formula. The same intervention can be applied across populations, regardless of context.
That shift aligned almost perfectly with the conditions already in place in large parts of Asia, where colonial administration, military provisioning, and institutional feeding programs had reduced diets to their simplest form. Polished rice, stripped of variability, became the baseline. It was uniform, storable, and easy to distribute. Within that system, adding a manufactured compound was far more profitable than rebuilding a diverse food supply.
Once introduced, the model expanded quickly. Fortification moved from a targeted response to a standardized practice. Supplementation followed, not as an emergency measure but as a routine part of daily life. The same framework that had been used to explain beriberi was applied again and again: identify the deficiency, isolate the compound, manufacture the solution, distribute it broadly.
Over time, this created a feedback loop. The more the system relied on processed and stabilized foods, the more it depended on adding back what had been removed. The more deficiencies that were identified, the stronger the justification for expanding production became.
Build Back Better
This is where the economic dimension becomes unavoidable. A model built on identifying widespread deficiencies naturally supports a system designed to correct them, especially when that system is scalable and profitable. The global market for fortified foods and vitamin supplementation grew accordingly, becoming a multi-billion-dollar industry that continues to expand year over year. What had started as a medical response became a permanent feature of the food and health economy.
Once the compound later called Thiamine was isolated, defined, and synthesized by the mid-1930s, the direction of the entire system shifted almost immediately. What had existed as part of a complex food structure was reduced to a single chemical input, and once that input could be manufactured, the race was on.
Companies like Merck & Co. were built to do one thing: take a compound, reproduce it through controlled chemical processes, and scale it. By 1936, thiamine had already been synthesized, and within a very short period, it was being produced commercially.
The Control and Monetization of the Food Supply
This is where fortification enters, not as a side note, but as the core of the con. Grains, cereals, processed foods, animal feed, all of it could be standardized, stripped down, and then rebuilt with specific chemical additions. The same compounds used in pharmaceutical production were now being added directly into food, not as medicine, but as a requirement. Take a moment to think about this. Not only do you have a cheap-to-make, no supply chain issue product, but you also have something governments REQUIRE their populations to consume in certain foods.
This chemical gold rush now expands into every category it can touch. Human food, livestock feed, infant formula, pharmaceutical products like IVs and medical nutrition products, and supplements. The same premix logic, the same controlled inputs, the same measurable outputs.
A system where food is expected to be incomplete without chemical correction. A system where the solution depends on the continued existence of the problem. A system where production, policy, and profit all align around maintaining that relationship.
The Chemical Soup We Call Thiamine
Once Thiamine moved into full industrial production, it stopped being something tied to food and became something built step by step through chemical synthesis. Synthetic thiamine is produced by assembling two primary structural components—a pyrimidine ring and a thiazole ring—through a multi-stage process built on basic chemical feedstocks such as acrylonitrile, methanol, and ammonia. These are not food-derived inputs; they are foundational industrial chemicals used across a wide range of manufacturing processes.
The first stage involves building the pyrimidine component. This typically uses methanol, ammonia, sodium methoxide, and acrylonitrile derivatives-you know, the good-for-you chemicals. Through controlled reactions, compounds such as 4-amino-5-ethoxymethyl-2-methylpyrimidine are formed, which smell so good when you cook them at home. This step often relies on condensation reactions involving intermediates such as malononitrile or acetamidine, which provide the backbone's nitrogen-rich structure.
The second stage constructs the thiazole component, which contains sulfur. This portion of the molecule is formed using compounds such as gamma-chloro-gamma-acetyl propanol, ammonia, and carbon disulfide. These reactions produce 5-(2-hydroxyethyl)-4-methylthiazole, completing the second half of the molecule. Easy as banana pancakes on a Sunday morning.
Once both components are formed, they are chemically combined in a coupling step, often called a quaternization reaction. This reaction is typically carried out in the presence of an acid, such as hydrochloric acid, which facilitates the formation of the thiamine backbone by linking the two ring structures.
The final stages involve “purification” and conversion into a stable, usable form. The crude product is processed using additional reagents, including hydrochloric acid and sodium hydroxide, to form thiamine hydrochloride, or further converted into thiamine mononitrate for improved stability in fortified foods. The end product is a white crystalline powder designed for consistency in manufacturing, storage, and distribution.
This is the form of thiamine that enters the food system through fortification and supplementation as a standardized compound produced through industrial chemistry and added back into processed products at defined levels.
Today, fortification and supplementation are not temporary measures; they are built into the design of the modern food supply. Intake of specific compounds is tracked, adjusted, and standardized across populations, while broader variables—how food is produced, how it degrades, and how individuals differ in their ability to process what they consume—are far more difficult to account for within the same system.
Because thiamine was not the end of this story. It was the beginning.
The same pattern, identify, isolate, reproduce, and deploy, did not stop at B1. It expanded across the entire B complex, each compound introduced with its own narrative, its own function, and its own place in the growing system of fortification and supplementation. Each addition reinforced the model, and each expansion extended its reach deeper into the food supply and into daily life.
What has not been fully examined is how those compounds interact when they are consumed together, repeatedly, and outside the context in which they originally existed. Nor has there been a complete accounting of how the shift from whole food systems to isolated inputs has altered the body's response over time.
That is where this investigation goes next.
Because once you start looking at the B vitamins as a group—how they are produced, how they are combined, and how they are delivered across multiple sources—the picture becomes far more complex than the individual stories can tell.
And some of what emerges will shock even the most seasoned of conspiracists.
References
Carpenter, K. J. (2000). Beriberi, white rice, and vitamin B: A disease, a cause, and a cure. University of California Press.
Combs, G. F. (2012). The vitamins: Fundamental aspects in nutrition and health (4th ed.). Academic Press.
Darnton-Hill, I., & Nalubola, R. (2008). Fortification strategies to meet micronutrient needs: Successes and failures. Proceedings of the Nutrition Society, 61(2), 231–241.
Everyday Health. (2023). Vitamin B1 (thiamine) overdose: Symptoms and side effects.
Food and Agriculture Organization. (2019). Guidelines on food fortification with micronutrients. FAO.
Fortune Business Insights. (2025). Fortified foods market size and future outlook report (2025–2034).
Grand View Research. (2021). Thiamine market size, share & trends analysis report (2021–2030).
Institute of Medicine. (1998). Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline. National Academy Press.
National Institutes of Health, Office of Dietary Supplements. (2022). Thiamin fact sheet for health professionals.
Ullmann’s Encyclopedia of Industrial Chemistry. (2012). Thiamine. Wiley-VCH.
U.S. Food and Drug Administration. (2020). Food standards: Enrichment and fortification of grains.
U.S. Pharmacist. (2023). Hypervitaminosis: A global concern.
Williams, R. R. (1936). The structure and synthesis of thiamine (vitamin B1). Journal of the American Chemical Society, 58(6), 1063–1065.
Williams, R. R., & Cline, J. K. (1936). Synthesis of vitamin B1. Journal of the American Chemical Society, 58(8), 1504–1505.
Disclaimer
The views expressed in this article are the author’s opinions, based on clinical experience, historical sources, public records, and secondary reporting. Where applicable, references to peer-reviewed and archival material are provided to support discussion of physiology and public health policy.
The author is a licensed Registered Nurse (RN) no longer working in the field. This article reflects professional observation and analysis, but it is not intended as individualized medical advice, diagnosis, or treatment. Readers should consult their own licensed healthcare professionals for personal medical decisions.
This piece is written for informational and educational purposes only. It does not allege proven legal wrongdoing by any named company or individual.
If you believe this article contains a factual error, or if you represent an entity mentioned and wish to provide source documentation or request a correction, please contact robin@purifywithin.com. Corrections will be made promptly where warranted.
Nothing in this article should be construed as medical or legal advice. For legal guidance regarding publishing, liability, or defamation, consult a qualified attorney.

![Magnesium Vs. Zinc The Battle Royale That Ends the Debate [By Medicine Girl]](https://dropinblog.net/cdn-cgi/image/fit=scale-down,format=auto,width=700/34264201/files/featured/94577ece-6b84-4d7c-b622-6e764231d715.png)