
Introduction
By now, the pHARMaceutical pattern should be impossible to unsee. This series did not begin because vitamins are cute little nutrients sitting quietly inside food. It began because the modern vitamin industry has trained the public to believe that synthetic chemical isolates are the same as whole, living nutrition, that deficiency stories explain everything, and that any symptoms produced after taking these compounds must mean the body needs even more of them. That belief system is the real product that the corporate giants are after.
We started with the early deficiency disease model, where industrial medicine learned how powerful it was to connect human suffering to a missing chemical and then sell the replacement back to the public. We moved into the manufacturing side, where synthetic B vitamins were no longer coming from industrial chemistry, fermentation tanks, fake patented organisms, chemical precursors, acids, solvents, catalysts, and mass-production systems built for profit and scale.
Then we entered the neurological vitamins, where the story became much harder to dismiss: B6, marketed for nerve support, has been linked to permanent neuropathy, burning sensations, numbness, ataxia, and long-term nerve dysfunction, while biotin, sold as beauty support, can interfere with laboratory tests strongly enough to distort thyroid panels, hormone testing, cancer markers, and even cardiac troponin results used in suspected heart attacks. Imagine how many false diagnoses have destroyed otherwise healthy people who should have simply stopped the offending poison and instead were sent down a road of misdiagnosis, pain, and suffering. I can’t help but wonder who would profit from such a common occurrence and could certainly 10-100X their initial investment in the vitamin tablets.
Hopefully, this will have shattered the innocent “water-soluble vitamins are harmless” narrative on the spot. This is one of the most important contradictions in the entire vitamin industry: the public is told that B vitamins are water-soluble, which creates the impression that the body simply uses what it needs and urinates out the rest. That sounds comforting, simple, and above all, safe. But if that were the whole truth, then why are “water-soluble” B vitamins building up in the body and producing documented toxicity patterns, neurological damage, dangerous diagnostic interference, and reactions severe enough to trigger regulatory warnings?
The industry loves the phrase “water-soluble” because it makes these compounds sound self-limiting. But solubility is not the same thing as harmlessness. A compound can dissolve in water and still accumulate in the tissues, alter enzymes, nerves, blood chemistry, laboratory assays, neurotransmitter pathways, methylation systems, hormone interpretation, and cellular signaling before the body manages to eliminate it. Water-soluble does not mean biologically irrelevant and incapable of harm.
The final vitamins in this series move into the most intimate territory yet. B8, B9, and B12 are not randomly grouped together. They sit at the center of the modern methylation, fertility, pregnancy, blood, brain, nerve, and genetic marketing machine. These are the compounds used to sell people on the chemical management of mood, reproduction, fetal development, fake DNA synthesis, red blood cell formation, psychiatric symptoms, fatigue, anxiety, fake “poor methylation,” MTHFR mutations, and lifelong biochemical optimization.
This article is not just about B8, but how the vitamin industry moved from selling deficiency prevention to selling chemical access to fertility, pregnancy, blood, brain, genes, mood, and identity itself. But of course, first you need to make your population devoid of all of their innate healthy characteristics and then sell them the cure. Just like they did with Polio, which somehow half of you can see, and parade your knowledge like a proud PhD graduate, but with the vitamins you turn into a demon, clawing at anyone trying to take away your vitamin binky.
B8: The Vitamin That Got Kicked Out of the Vitamin Club but Still Gets Sold Like One
If the vitamin classification system hasn’t already started looking ridiculous, it most certainly will now. Most people have never heard of B8, and if they have, they usually know it as inositol. The story begins in the 1800s, when myo-inositol was first isolated from muscle extracts by German chemist Johannes Joseph Scherer in 1850. The name itself derives from its early association with muscle tissue, and for a time, it was grouped with the expanding B-vitamin complex as “Vitamin B8.” Later, once researchers saw that the body synthesized it and that it did not meet the strict definition of an essential vitamin, it was quietly removed from the official vitamin category, but the story doesn’t end there. They still have a potential gold mine, just not quite as lucrative as they once hoped. As you can see, it is even a cure for bickering with your spouse so you both can fall in love again. Ahhh, of course it is.

Inositol is a compound found in the body. Of course, they have to perpetuate the myth that the compounds are somehow found hidden inside foods, especially fruits, beans, grains, nuts, and seeds. In plants, it is often hidden in phytate forms, which adds another layer of nutritional smoke and mirrors confusion, because phytates can allegedly bind minerals and reduce mineral absorption depending on the food matrix and preparation. Similar to Vitamin D3, the fat-soluble vitamin that binds and captures minerals from your bones.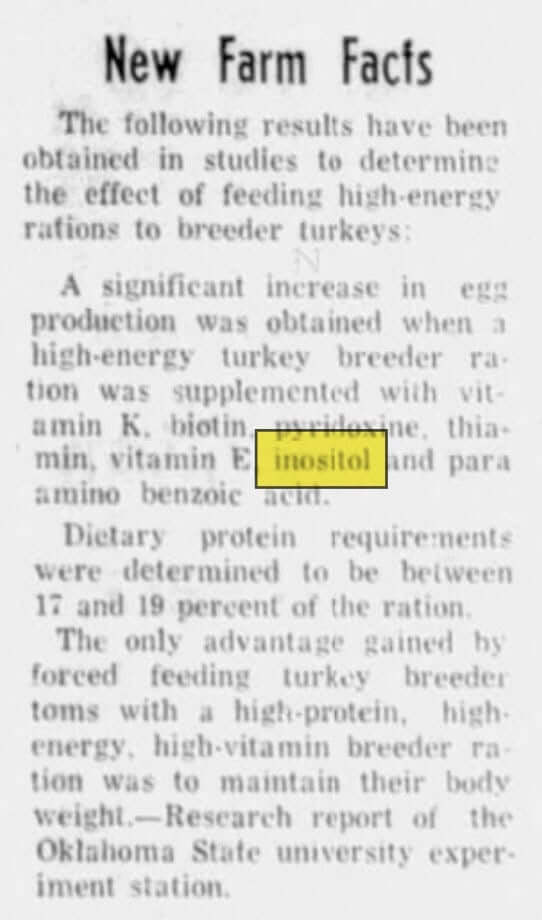
And here is where the B8 story gets even more revealing. The research itself admits that myo-inositol was “for a long time” considered Vitamin B8, but is no longer considered an essential nutrient because the body forms it from glucose. At the same time, the same paper describes myo-inositol as deeply involved in insulin signaling, hormone signaling, cell membrane function, peripheral nerve development, reproduction, osmoregulation, ovarian function, and glucose metabolism. That is a strange little trick. Officially, it is removed from the essential vitamin category, but functionally, it is still treated identically—like a biochemical lever in some sensitive hormone systems in the body.
The brain concentrates myo-inositol at levels reported to be 10 to 15 times higher than blood, while the kidneys produce around 2 grams per day and also play a major role in handling and breaking it down. The kidneys, reproductive organs, brain, blood cells, semen, breast milk, and nervous tissue all have meaningful relationships with inositol. Elevated glucose can reduce inositol uptake into tissues, increase urinary losses, and deplete inositol in nervous tissue. In other words, the entire sales pitch around PCOS, diabetes, insulin resistance, and metabolic syndrome rests on the idea that modern glucose dysregulation disrupts inositol handling. The industry then turns around and sells isolated inositol as the answer to a metabolic problem that is likely rooted in the same modern food, chemical, stress, and endocrine-disrupting environment the supplement industry conveniently ignores.
This is where PCOS becomes the perfect sales funnel. PCOS affects an ever-growing percentage of women of reproductive age, and insulin resistance is common in PCOS, including in lean women. It describes how hyperinsulinemia can increase ovarian androgen synthesis and disrupt ovarian signaling, while myo-inositol and D-chiro-inositol act as secondary messengers in insulin pathways. That is the official mechanism used to justify selling inositol for PCOS: if insulin signaling is disrupted, give the body more of the compound involved in that signaling.
But that explanation skips the question women actually deserve answered: why are so many women developing insulin resistance, ovarian dysfunction, androgen excess, irregular cycles, fertility issues, and metabolic chaos in the first place? Instead of confronting the wider environment — processed food, massive amounts of food industry endocrine disruptors, synthetic hormones, stress physiology, fortified products, medications, industrial oils, glucose overload, and chronic chemical exposure- the market narrows the problem down to a pathway and sells a powder to push that pathway.
The industry uses myo-inositol as a preferred treatment for major metabolic disorders, stating that it may lower serum insulin and improve insulin resistance approximately twofold better than pioglitazone or metformin in patients with impaired glucose tolerance. Metformin and pioglitazone are prescription drugs used to alter glucose metabolism. If inositol is being discussed in the same breath as those drugs for insulin resistance, then the public needs to stop pretending this is not just a sleeper vitamin, but a prescription drug with similar negative side effect protocols.
When a “Vitamin” Acts Like a Drug but Sells Like a Supplement
This is where B8 becomes more revealing than almost any official vitamin. Inositol was removed from the essential vitamin category because the body can make it, yet it is still sold as if people need to take it from the outside to correct mood (does that at least raise one or two red flags?) hormones, ovulation, insulin signaling, fertility, metabolic dysfunction, and even pregnancy-related glucose issues. So what exactly is it? If it is not essential enough to remain a vitamin, but powerful enough to alter insulin signaling, ovarian function, neurotransmitter pathways, and metabolic markers, then the public deserves a better word than “support.”
Inositol is discussed in the literature as part of insulin signaling and second-messenger pathways. That means it is being used to influence communication systems inside the body, which is why it gets compared to metabolic drugs like metformin and pioglitazone in PCOS and insulin-resistance discussions. Those drugs are prescribed because they alter glucose metabolism. Inositol is marketed because it alters glucose metabolism. The mechanism is not identical molecule-for-molecule, but what possibly could you convince any logical person of the difference? They increase insulin sensitivity, interfere with metabolic signaling, interfere with ovulation, and change downstream hormonal patterns.
That raises the obvious question: if inositol is being used pharmaceutically, why is it not treated like a drug? The answer is not hard to see. If inositol were pushed fully into the pharmaceutical category, the rules would change. Companies would face a more expensive approval pathway, stricter claims, tighter dosing standards, adverse-event monitoring, prescription control, liability exposure, and far less freedom to market it casually to millions of women online. The supplement category gives the industry a better deal and higher degree of profit. It allows companies to sell a pharmacologic treatment while using soft language: “supports ovarian health,” “supports insulin balance,” “supports mood,” “supports fertility,” “supports metabolic wellness.” The word “support” becomes the legal disguise that lets a biochemical intervention slip into the supplement category. There is no difference, except for the words slapped on it.
That is the business genius of B8. As a prescription drug, inositol would have to compete with existing metabolic drugs, fertility drugs, diabetes drugs, and hormone-management protocols. As a supplement, it can sit beside them, under them, around them, and before them. It does not have to replace metformin to become profitable. It can become the “natural” add-on to the pharmaceutical hesitant, the pre-drug option, the fertility-clinic recommendation, the influencer protocol, the PCOS starter pack, the wellness powder women buy before they ever reach the prescription pad. That is how a declassified vitamin becomes a multimillion-dollar product without needing to slip into the pharmaceutical cage. And if you own both sides of the industry? Then you believe you are more powerful than God and nothing can stop you and your diabolical plan.
And yes, health care salesmen clinicians do recommend it. Inositol is discussed in PCOS research, fertility medicine, metabolic syndrome, gestational diabetes, mood disorders, and insulin resistance. Some physicians, fertility specialists, dietitians, naturopaths, and functional-medicine providers recommend myo-inositol or myo-inositol/D-chiro-inositol combinations, especially for PCOS patients. It shows inositol has crossed into therapeutic use while still benefiting supplement freedom from regulation.
This is the loophole no one knows. If a compound is called a drug, people become cautious. If it is called a vitamin or a supplement, people self-dose. B8 exploited both worlds without fully belonging to any of them. It luckily lost the official vitamin label, avoided the full burden of drug regulation, and landed in the most profitable lane possible: a wellness product with drug-like promises, sold to desperate women through the language of natural support.
That is how the pipe dream became the product. Not because the public suddenly developed a classic inositol deficiency disease from something their body makes. Not because women’s ovaries forgot how to function. No, it is much more simplistic. They found a way to turn a profit.
The dosing makes the “just nutrition” argument fall apart. Common PCOS protocols often use 2 grams of myo-inositol twice daily, or about 4 grams per day, sometimes combined with D-chiro-inositol in a 40:1 ratio. Gestational diabetes studies have also used 2 grams twice daily. Metabolic syndrome discussions commonly land around 2 grams per day or higher. Psychiatric trials have gone even further, using 12 grams per day for depression and panic disorder, and some panic-disorder studies have used doses up to 18 grams per day. These are not incidental food exposures. These are therapeutic gram-level interventions being used to push signaling systems.
That is the angle that made B8 profitable. If inositol were treated like a pharmaceutical, companies would face stricter claims, tighter dosing standards, adverse-event monitoring, liability exposure, and far less freedom to market it casually to millions of people. The supplement category gives sellers the better deal: imply therapeutic benefit while hiding behind softer language like “supports ovarian health,” “supports insulin balance,” “supports mood,” “supports fertility,” and “supports metabolic wellness.” It does not need to replace metformin, fertility drugs, diabetes drugs, psychiatric drugs, or hormone protocols. It only needs to sit beside them as the “natural” add-on, the pre-drug option, the fertility-clinic suggestion, the metabolic powder, and the influencer-approved protocol. That is how a declassified vitamin became a multimillion-dollar product: it lost the official vitamin label, avoided the full drug label, kept the therapeutic promise, and landed in the most profitable lane possible.
The Ruse
And then comes the industry tell. The authors of a Myo-inositol for Insulin Resistance, Metabolic Syndrome, Polycystic Ovary Syndrome, and gestational diabetes disclose competing interests: one author is the director of scientific affairs at AIDP and is affiliated with companies that sell myo-inositol, while the other owns a supplement company. That absolutely matters when the article concludes that myo-inositol should be considered for insulin resistance, metabolic syndrome, diabetes, PCOS, and gestational diabetes. When the people writing the glowing review are tied to the industry or, in this case, the supplement market, then, ladies and gentlemen, we have the definition of science as it has come to be known.
So B8 becomes one of the cleanest examples of the new vitamin economy. The industry needs to be one step ahead. They know that eventually the dam of lies will break, and even the densest of all dense folks will figure out we do not have a synthetic chemical deficiency, that they have been played by a trillion-dollar industry. So, it does not need to remain an official vitamin to remain profitable; it only needs a pathway, a population of desperate women, a few metabolic markers, and a market trained to believe every symptom is a supplement opportunity. It is sold to women trying to regulate their cycles and conceive babies. It is placed into formulas and wellness blends. It is used in nutraceutical products aimed at anxiety, mood, insulin resistance, and metabolic health. It is pushed into animal nutrition because the inositol-phytate-phosphorus relationship affects feed efficiency, mineral handling, and growth economics. The same molecule moves through fertility clinics, supplement brands, infant nutrition, livestock production, and industrial ingredient supply chains while the public is still being handed the soft little word “support.”
By the 1930s, inositol was already being discussed as commercially useful beyond its nutritional uses. Researchers were exploring ways to extract it from corn-processing waste, and inositol nitrate was even discussed in relation to explosives chemistry because of its relationship to nitro compounds.
Today, inositol shows up in several markets at once. It is still sold as a dietary supplement, just not labeled B8, used in women’s health formulas, fertility protocols, PCOS products, mood and anxiety supplements, metabolic support blends, and sometimes prenatal-adjacent products. It is also used in animal nutrition and feed-related industries because of the inositol/phytate/phosphorus relationship when manufacturers are trying to manipulate growth, mineral handling, and feed cost. Once again, the same compound family moves through human supplements, animal production, food processing, fertility marketing, and industrial chemistry.
And the money confirms why this molecule never really disappeared after being kicked out of the official vitamin club. The global inositol market is now valued at hundreds of millions of dollars, with projections indicating continued growth over the next decade. According to market reports, the Vitamin B8/inositol sector is estimated to exceed $400 million, with projected annual growth rates often ranging from 6.5% to 9% through 2031. That growth is not being driven by some rare deficiency disease. It is being driven by the modern wellness machine: women’s health, PCOS, fertility, hormonal support, mental wellness, metabolic syndrome, infant nutrition, and animal feed. And of course, everyone knows modern medicine will not cure any of these diseases because they caused them in the first place, in my opinion.
The major players are not cottage-kitchen herbalists grinding seeds in a mortar. This market involves global chemical, biotechnology, pharmaceutical, and ingredient companies competing over purity, production efficiency, supply chains, sustainability claims, and branded ingredient positioning. Companies such as DSM, BASF, Shandong Runde Biotechnology, and Zhucheng Haotian Pharm are part of the broader industrial ingredient landscape around inositol production and supply.
The standard system often moves women from birth control to metformin to fertility drugs to hormone panels to endless monitoring. Then the supplement industry slides in with the “natural” version of the same management model for those resistant to pharmaceuticals.
And the direct effects of taking the drug? High-dose inositol at larger doses, especially above 12 grams per day, can cause diarrhea, nausea, gas, and digestive distress, which are the direct effects of taking poison. Because it can influence insulin signaling and glucose handling, it may also increase the risk of hypoglycemia when combined with diabetes medications or other glucose-lowering agents. Psychiatric cautions have also appeared, including some reports of manic or hypomanic reactions in people with bipolar disorder and concerns in severely depressed patients. Pregnancy is another area where the messaging becomes slippery: while some low-dose studies in gestational diabetes report no major adverse events, older cautions warn against late-pregnancy use because of possible uterine contractions. Even in fertility marketing, the story is not clean. Myo-inositol and D-chiro-inositol are not interchangeable, and improper ratios or overuse have been criticized by fertility experts, with some concern that excessive D-chiro-inositol may worsen ovarian response or egg quality in certain cases.
Conclusion
B8 is the perfect ending point for this article because it offers a different angle on the vitamin industry. This is not the classic deficiency story. There is no dramatic B8 deficiency disease haunting the public imagination. There is no clean textbook villain like scurvy or beriberi. There is a compound that was once called a vitamin, later removed from the official essential vitamin category, and then quietly absorbed into the modern wellness economy anyway.
That should tell people everything they need to know about how flexible these labels really are. They are pharmaceuticals, by any other name would sell just as toxic.
Once the industry found a way to connect it to insulin signaling, PCOS, fertility, mood, anxiety, metabolic syndrome, gestational diabetes, infant nutrition, and animal feed, the old vitamin label became almost irrelevant. The money was already moving.
The most disturbing part is how neatly B8 fits into the new model of health management. The old vitamin industry sold deficiency. The newer version sells optimization. Better cycles. Better fertility. Better mood. Better insulin response. Better calm. Better hormones. Better metabolic function. But first you need everyone suffering from illness and disease. The promise is always improvement, but the mechanism remains biochemical interference via an isolated compound, at doses that have nothing to do with the food matirx.
Women became the perfect target because PCOS, infertility, irregular cycles, anxiety, weight changes, and hormonal symptoms are emotionally loaded, poorly explained, and easy to monetize. Instead of asking why so many women are developing metabolic and reproductive dysfunction in the first place, the market narrows the conversation to a pathway and sells a powder to push that pathway. The woman is told her body needs support, while the larger system that disrupted her body escapes interrogation. That is the real lesson of B8.
A compound can be manufactured through industrial extraction, chemical processing, or microbial fermentation and still be marketed as natural. It can be used in fertility formulas, infant nutrition, animal feed, metabolic protocols, and psychiatric-adjacent products while still being described with wellness language. It can be discussed in research alongside prescription metabolic drugs, while consumers are told it is just a OTC supplement you can try. You know, the good guys.
At some point, the public has to start asking what it is doing inside the body. B8 reveals the bridge between the old deficiency racket and the modern optimization racket. The industry no longer needs a classic deficiency disease to sell lifelong supplementation. It only needs vague symptoms, a biochemical pathway, a vulnerable population, and enough scientific language to make intervention sound like “essential” nourishment.
It proves the vitamin label was never as stable, innocent, as people were taught to believe. And if a forgotten, declassified “vitamin” can become a multimillion-dollar fertility, mood, metabolic, infant nutrition, and animal-feed ingredient, then the next question becomes much darker.
What happens when the same machine moves into pregnancy itself?
Folic acid is the door they do not want opened. The next article follows B9 from anemia research and spinach leaves into synthetic chemistry, mandatory fortification, prenatal fear, MTHFR marketing, unmetabolized folic acid, B12 masking, cancer questions, and the billion-dollar machinery built around mothers, babies, and genetic anxiety. This is where the B-vitamin story becomes our darkest nightmare.
References
Bizzarri, M., Carlomagno, G., & Unfer, V. (2011). Inositol: History of an effective therapy for polycystic ovary syndrome. European Review for Medical and Pharmacological Sciences, 15(2), 1896–1903.
Cleveland Clinic. (2023). Inositol: Benefits & side effects. Cleveland Clinic.
DiNicolantonio, J. J., & O’Keefe, J. H. (2022). Myo-inositol for insulin resistance, metabolic syndrome, polycystic ovary syndrome and gestational diabetes. Open Heart, 9(1), e001989.
Han, P., Zhang, L., Luo, X., Chen, Y., Li, X., & Liu, J. (2023). High-titer production of myo-inositol by a co-immobilized multi-enzyme system. Chemical Engineering Journal, 466, 143177.
Irvine, R. F. (2016). A short history of inositol lipids. Journal of Lipid Research, 57(11), 1987–1994.
López-Gambero, A. J., Sanjuan, C., Serrano-Castro, P. J., Suárez, J., & Rodríguez de Fonseca, F. (2020). The biomedical uses of inositols: A nutraceutical approach to metabolic dysfunction in aging and neurodegenerative diseases. Biomedicines, 8(9), 295.
Mellonie, P., Sharma, S., & Singh, S. (2024). The effectiveness of myo-inositol in women with polycystic ovary syndrome: A systematic review. Cureus, 16(3), e56218.
National Center for Biotechnology Information. (2024). Inositol. PubChem Compound Summary.
Showell, M. G., Mackenzie-Proctor, R., Jordan, V., Hodgson, R., & Farquhar, C. (2018). Inositol for subfertile women with polycystic ovary syndrome. Cochrane Database of Systematic Reviews, 2018(12), CD012378.
Yi, M., Zhang, X., Li, Y., & Wang, Z. (2020). Biosynthesis of myo-inositol in Escherichia coli by engineering glucose metabolism. Materials Today Communications, 25, 101591.

![The Great Vitamin Liars Vitamins [Part 1 By Medicine Girl]](https://dropinblog.net/cdn-cgi/image/fit=scale-down,format=auto,width=700/34264201/files/featured/0c2c0703-aac4-4a09-8bbb-aa55f98bf33e.png)


![Magnesium Vs. Zinc The Battle Royale That Ends the Debate [By Medicine Girl]](https://dropinblog.net/cdn-cgi/image/fit=scale-down,format=auto,width=700/34264201/files/featured/94577ece-6b84-4d7c-b622-6e764231d715.png)

